

Improved Right Ventricular Diastolic Function Assessed by Hepatic Vein Flow After Pectus Excavatum Repair
- PMID: 39790315
- PMCID: PMC11708325
- DOI: 10.1016/j.atssr.2023.02.009
Improved Right Ventricular Diastolic Function Assessed by Hepatic Vein Flow After Pectus Excavatum Repair
Abstract
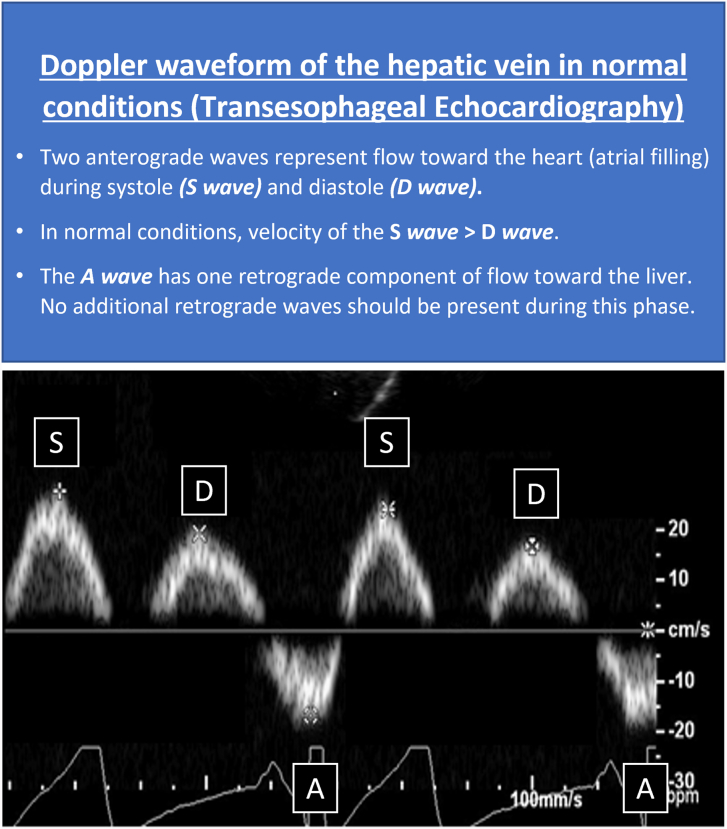
Background: The cardiovascular benefits of surgical repair in pectus excavatum (PEx) continue to be debated, with limited data supporting repair in adult patients. Hepatic vein flow is used to identify right-sided diastolic dysfunction in cardiovascular disorders, including tricuspid stenosis, cardiac tamponade, and constrictive pericarditis. This study evaluates the effects of cardiac compression on diastolic function (as assessed by hepatic vein flow patterns and velocities) before and after repair of PEx.
Methods: A retrospective study was performed of intraoperative transesophageal echocardiograms including hepatic vein assessments of adult patients who underwent preoperative and postoperative evaluations during repair of PEx from 2018 to 2021.
Results: In total, 127 patients were included (median age, 29.0 [15.4] years; median Haller index, 4.2 [1.7]; 60.6% male). Statistically significant improvements were seen after pectus repair of right ventricular stroke volume and diastolic function as measured by increased postoperative velocities for hepatic vein waves (P < .001 for all comparisons). Preoperatively, 5.5% of patients had constrictive-like physiology with end-diastolic retrograde flow that normalized postoperatively (P = .016). Approximately 10% of patients changed their pattern of hepatic vein flow after surgical procedure. Patients with more proximal cardiac compression had greater improvements in hepatic vein velocities after repair.
Conclusions: Surgical relief of cardiac compression resulted in an immediate improvement in hepatic vein flow and right ventricle stroke volume in patients with PEx. These results support diastolic dysfunction in a large number of patients, with improvement in function and compliance after the surgical relief of cardiac compression.
© 2023 The Authors.
Figures



References
-
- Rodriguez-Granillo G.A., Raggio I.M., Deviggiano A., et al. Impact of pectus excavatum on cardiac morphology and function according to the site of maximum compression: effect of physical exertion and respiratory cycle. Eur Heart J Cardiovasc Imaging. 2020;21:77–84. doi: 10.1093/ehjci/jez061. - DOI - PubMed
LinkOut - more resources
Full Text Sources
