

Case Reports
doi: 10.1016/j.atssr.2024.07.004.
eCollection 2024 Dec.
Endoluminal Wound Vacuum Therapy: A Paradigm Shift in Managing Esophageal Bronchial Fistula
Affiliations
- PMID: 39790607
- PMCID: PMC11708291
- DOI: 10.1016/j.atssr.2024.07.004
Item in Clipboard
Case Reports
Endoluminal Wound Vacuum Therapy: A Paradigm Shift in Managing Esophageal Bronchial Fistula
Ann Thorac Surg Short Rep.
.
Abstract
Esophageal bronchial fistula after Ivor Lewis esophagectomy is a challenging complication. Surgical treatment is definitive, but it carries high morbidity and mortality, whereas esophageal stents have been shown to be temporary measures. We highlight the case of a patient who was treated with endoluminal wound vacuum therapy. The fistula healed after 9 days of therapy. The likely reason for success was the presence of an omentum between the esophagus and the bronchus that was placed during esophagectomy and that provided adequate tissue to close the fistula. In a patient with appropriate anatomy, esophageal bronchial fissure can be successfully treated with endoluminal wound vacuum therapy.
© 2024 The Authors.
Figures
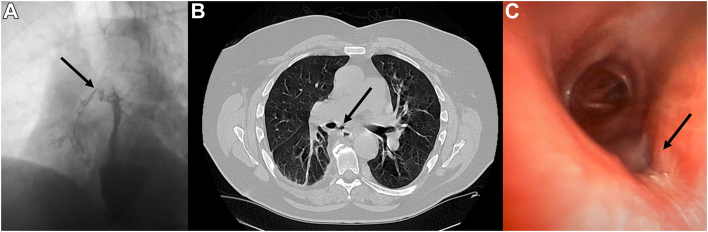
Esophagobronchial fistula. (A) Esophagogram showing contrast medium in the right main bronchus (arrow). Computed tomographic scan showing the fistula between the esophagus and the bronchus with the omentum (arrow) between them without a major vessel near the fistula. (C) Bronchoscopic image showing a 5-mm defect in the bronchus intermedius (arrow).
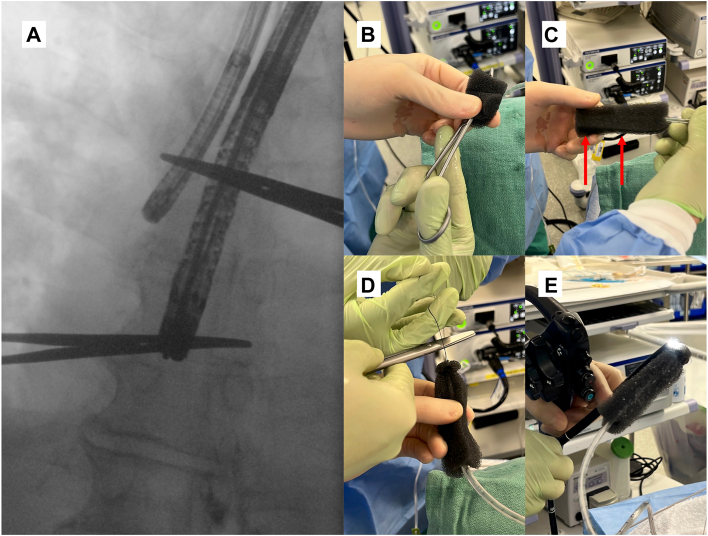
Endoluminal wound vacuum therapy. (A) The image shows the location of the defect in the bronchus with the tip of the bronchoscope and anastomosis marked by the endoscope. A vacuum sponge was cut to 10 cm × 2.5 cm × 3.2 cm. (B) We placed the hemostat in the middle and pulled the nasogastric tube through the sponge with the hemostat covering the side holes. (C) We sutured 3-0 silk through the sponge and the nasogastric tube and secured it in 2 places (marked by red arrows). (D) We sutured 2-0 nylon at the tip. (E) The nylon was held with a rat tooth grasper, which was pulled into the endoscope. The sponge was centered around the anastomosis.
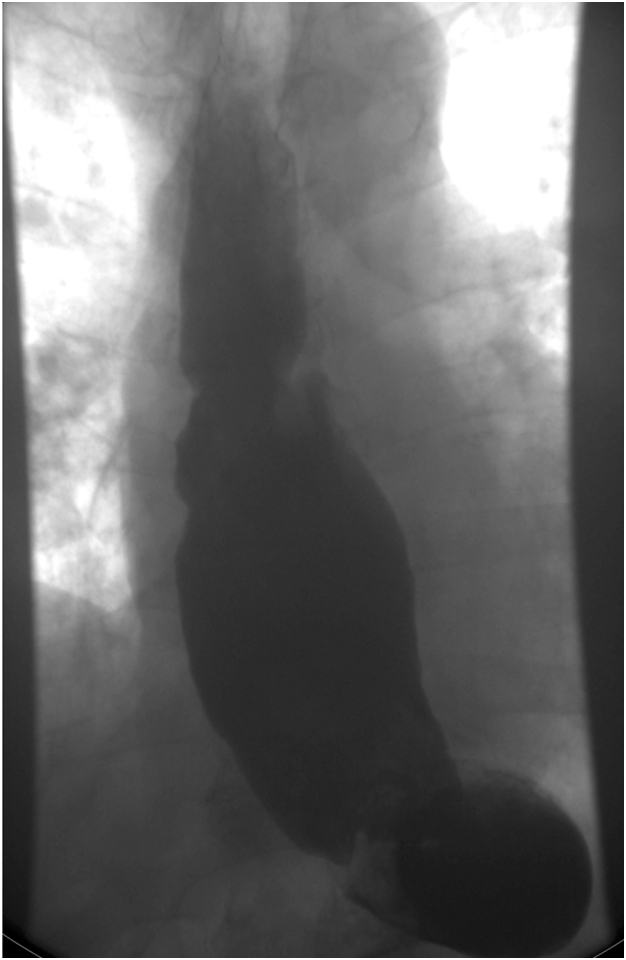
Barium esophagram showing resolution of the esophagobronchial fistula.
References
-
- Moore C.B., Almoghrabi O., Hofstetter W., Veeramachaneni N. Endoluminal wound vac: an evolving role in treatment of esophageal perforation. J Visc Surg. 2020;6 43-43.
Publication types
LinkOut - more resources
Full Text Sources
