

Development and Validation of a Deep Learning Model Based on MRI and Clinical Characteristics to Predict Risk of Prostate Cancer Progression
- PMID: 39792014
- PMCID: PMC11791668
- DOI: 10.1148/rycan.240078
Development and Validation of a Deep Learning Model Based on MRI and Clinical Characteristics to Predict Risk of Prostate Cancer Progression
Abstract
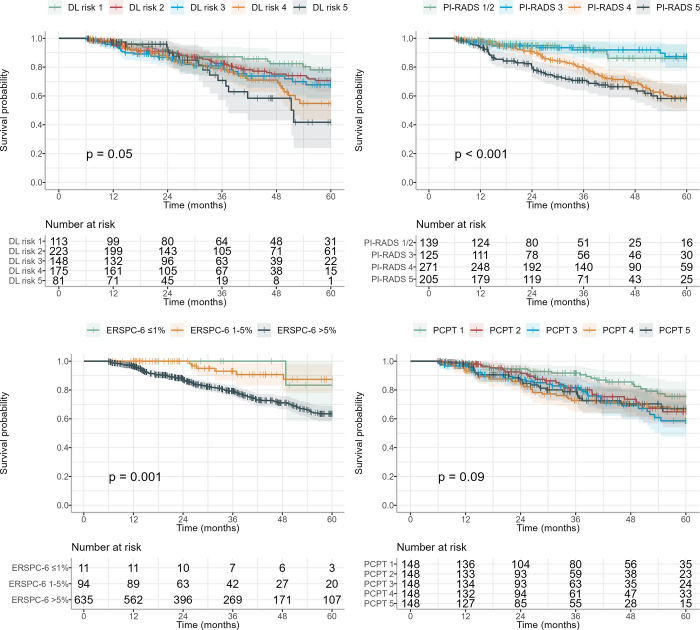
Purpose To validate a deep learning (DL) model for predicting the risk of prostate cancer (PCa) progression based on MRI and clinical parameters and compare it with established models. Materials and Methods This retrospective study included 1607 MRI scans of 1143 male patients (median age, 64 years; IQR, 59-68 years) undergoing MRI for suspicion of clinically significant PCa (csPCa) (International Society of Urological Pathology grade > 1) between January 2012 and May 2022 who were negative for csPCa at baseline MRI. A DL model was developed using baseline MRI and clinical parameters (age, prostate-specific antigen [PSA] level, PSA density, and prostate volume) to predict the time to PCa progression (defined as csPCa diagnosis at follow-up). Internal and external testing was performed. The model's ability to predict progression to csPCa was assessed by Cox regression analyses. Predictive performance of the DL model up to 5 years after baseline MRI in comparison with the European Randomized Study of Screening for Prostate Cancer (ERSPC) future-risk calculator, Prostate Cancer Prevention Trial (PCPT) risk calculator, and Prostate Imaging Reporting and Data System (PI-RADS) was assessed using the Harrell C-index. Optimized follow-up intervals were derived from Kaplan-Meier curves. Results DL scores predicted csPCa progression (internal cohort: hazard ratio [HR], 1.97 [95% CI: 1.61, 2.41; P < .001]; external cohort: HR, 1.32 [95% CI: 1.14, 1.55; P < .001]). The model identified a subgroup of patients (approximately 20%) with risks for csPCa of 3% or less, 8% or less, and 18% or less after 1-, 2-, and 4-year follow-up, respectively. DL scores had a C-index of 0.68 (95% CI: 0.63, 0.74) at internal testing and 0.56 (95% CI: 0.51, 0.61) at external testing, outperforming ERSPC and PCPT (both P < .001) at internal testing. Conclusion The DL model accurately predicted PCa progression and provided improved risk estimations, demonstrating its ability to aid in personalized follow-up for low-risk PCa. Keywords: MRI, Prostate Cancer, Deep Learning Supplemental material is available for this article. ©RSNA, 2025.
Keywords: Deep Learning; MRI; Prostate Cancer.
Conflict of interest statement
Figures




References
-
- Epstein JI , Egevad L , Amin MB , et al. . The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma: definition of grading patterns and proposal for a new grading system . Am J Surg Pathol 2016. ; 40 ( 2 ): 244 – 252 . - PubMed
-
- Chen RC , Rumble RB , Loblaw DA , et al. . Active surveillance for the management of localized prostate cancer (Cancer Care Ontario guideline): American Society of Clinical Oncology clinical practice guideline endorsement . J Clin Oncol 2016. ; 34 ( 18 ): 2182 – 2190 . - PubMed
-
- van den Bergh RC , Roemeling S , Roobol MJ , Roobol W , Schröder FH , Bangma CH . Prospective validation of active surveillance in prostate cancer: the PRIAS study . Eur Urol 2007. ; 52 ( 6 ): 1560 – 1563 . - PubMed
-
- Ahmed HU , El-Shater Bosaily A , Brown LC , et al. . Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): a paired validating confirmatory study . Lancet 2017. ; 389 ( 10071 ): 815 – 822 . - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
