

Estimated prevalence of post-intensive care cognitive impairment at short-term and long-term follow-ups: a proportional meta-analysis of observational studies
- PMID: 39792310
- PMCID: PMC11723879
- DOI: 10.1186/s13613-025-01429-z
Estimated prevalence of post-intensive care cognitive impairment at short-term and long-term follow-ups: a proportional meta-analysis of observational studies
Abstract
Objective: Evidence of the overall estimated prevalence of post-intensive care cognitive impairment among critically ill survivors discharged from intensive care units at short-term and long-term follow-ups is lacking. This study aimed to estimate the prevalence of the post-intensive care cognitive impairment at time to < 1 month, 1 to 3 month(s), 4 to 6 months, 7-12 months, and > 12 months discharged from intensive care units.
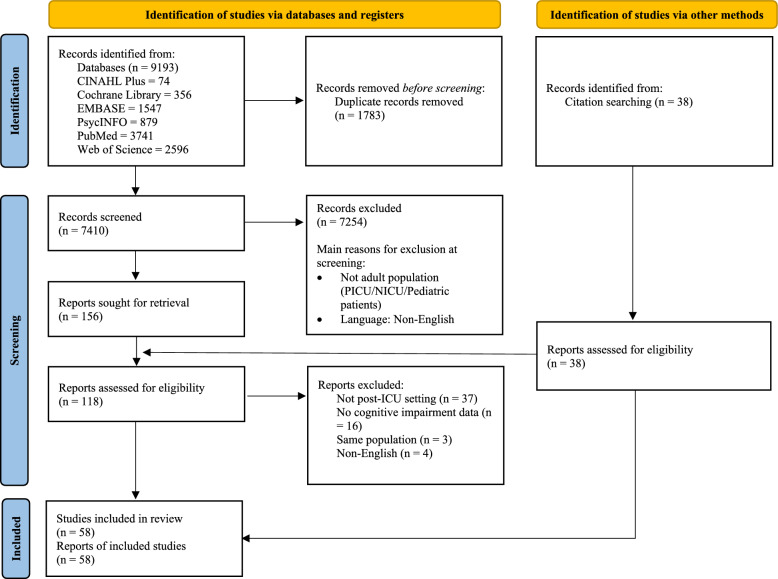
Methods: Electronic databases including PubMed, Cochrane Library, EMBASE, CINAHL Plus, Web of Science, and PsycINFO via ProQuest were searched from inception through July 2024. Studies that reported on cognitive impairment among patients discharged from intensive care units with valid measures were included. Data extraction and risk of bias assessment were performed independently for all included studies according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses reporting guidelines. Newcastle-Ottawa Scale was used to measure risk of bias. Data on cognitive impairment prevalence were pooled using a random-effects model. The primary outcome was pooled estimated proportions of prevalence of the post-intensive care cognitive impairment.
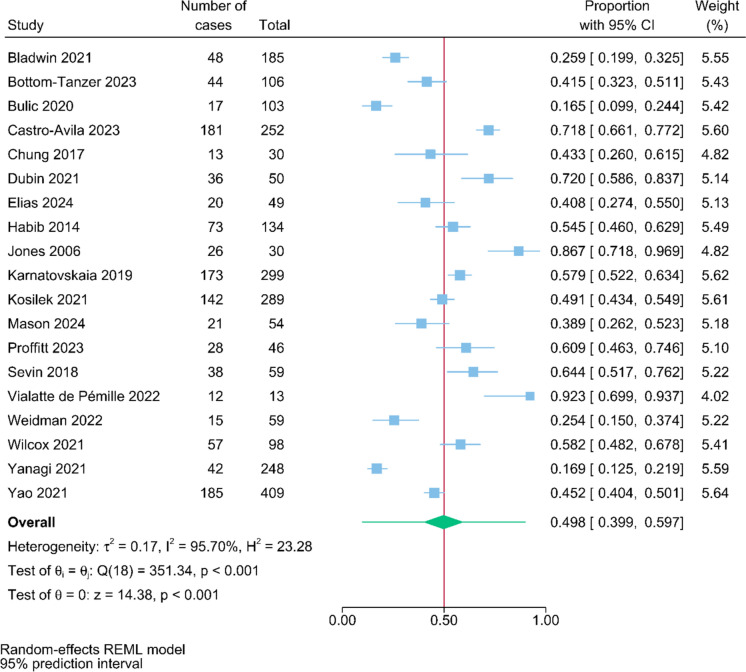
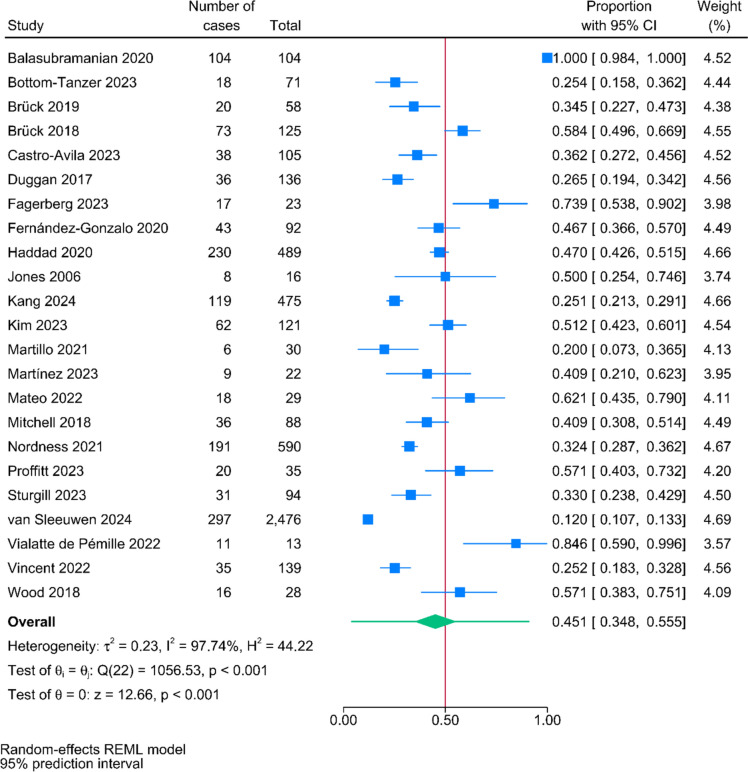
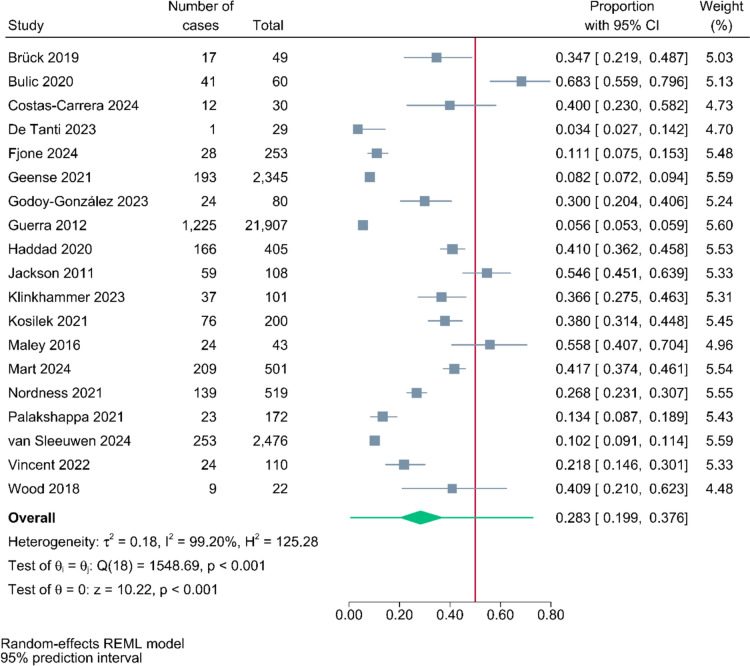
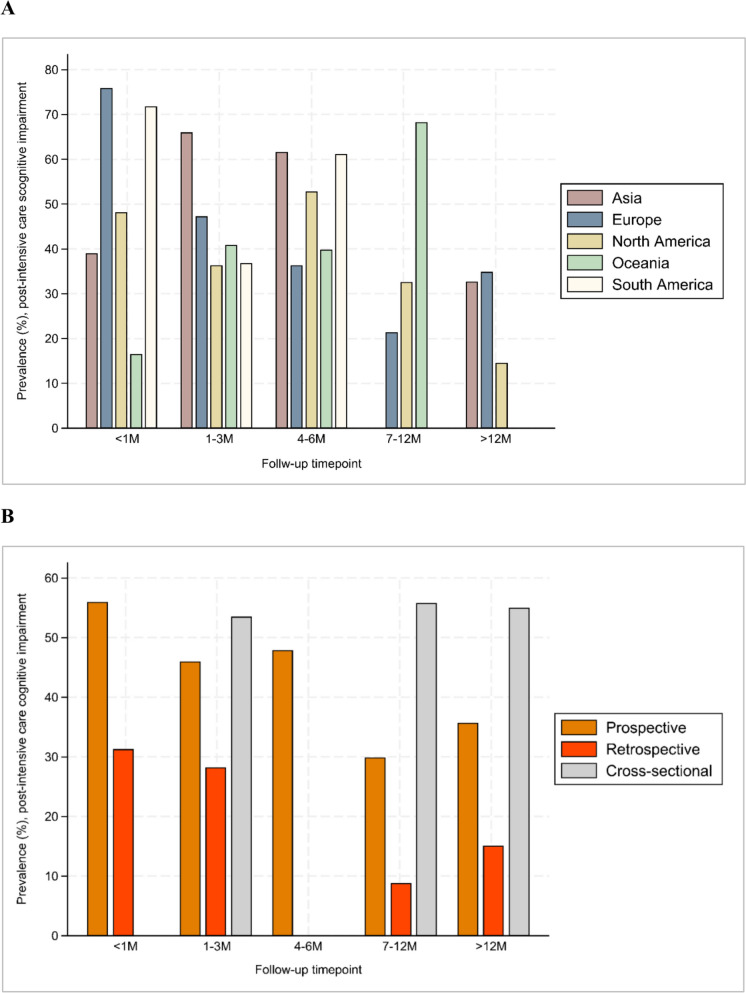
Results: In total, 58 studies involving 347,940 patients were included. The pooled post-intensive care cognitive impairment prevalence rates at the follow-up timepoints < 1 month, 1-3 month(s), 4-6 months, 7-12 months, > 12 months were 49.8% [95% Prediction Interval (PI), 39.9%-59.7%, n = 19], 45.1% (95% PI, 34.8%-55.5%, n = 23), 47.9% (95% PI, 35.9%-60.0%, n = 16), 28.3% (95% PI, 19.9%-37.6%, n = 19), and 30.4% (95% PI, 18.4%-43.9%, n = 7), respectively. Subgroup analysis showed that significant differences of the prevalence rates between continents and study designs were observed.
Conclusions: The prevalence rates of post-intensive care cognitive impairment differed at different follow-up timepoints. The rates were highest within the first three months of follow-up, with a pooled prevalence of 49.8% at less than one month, 45.1% at one to three months, and 47.9% at three to six months. No significant differences in prevalence rates between studies that only included coronavirus disease 2019 survivors. These fundings highlight the need for further research to develop targeted interventions to prevent or manage cognitive impairment at short-term and long-term follow-ups.
Keywords: Cognitive impairment; Critically ill survivors; Post-intensive care syndrome; Proportional meta-analysis; Systematic review.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable as this is a systematic review and meta-analysis. Consent for publication: Not applicable. Competing interests: Dr Mu-Hsing Ho reported receiving grant funding from the Health and Medical Research Fund (HMRF), Health Bureau, Hong Kong SAR and HMRF Research Fellowship Scheme, Health Bureau, Hong Kong SAR during the conduct of the study. No other disclosures were reported.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
