

Establishing a living biobank of pediatric high-grade glioma and ependymoma suitable for cancer pharmacology
- PMID: 39792378
- PMCID: PMC12187455
- DOI: 10.1093/neuonc/noaf007
Establishing a living biobank of pediatric high-grade glioma and ependymoma suitable for cancer pharmacology
Abstract
Background: Brain tumors are the deadliest solid tumors in children and adolescents. Most of these tumors are glial in origin and exhibit strong heterogeneity, hampering the development of effective therapeutic strategies. In the past decades, patient-derived tumor organoids (PDT-O) have emerged as powerful tools for modeling tumoral cell diversity and dynamics, and they could then help define new therapeutic options for pediatric brain tumors.
Methods: Through an integrative approach based on our expertise and a careful review of the literature about glioblastoma 3D primary cultures, we set up a standardized methodological pipeline for the establishment, characterization, and biobanking of PDT-O through direct 3D in vitro culture of the deadliest pediatric glial brain tumors. To assess PDT-O fidelity and validate their preclinical relevance, we performed comprehensive histological, molecular, and drug-response analyses.
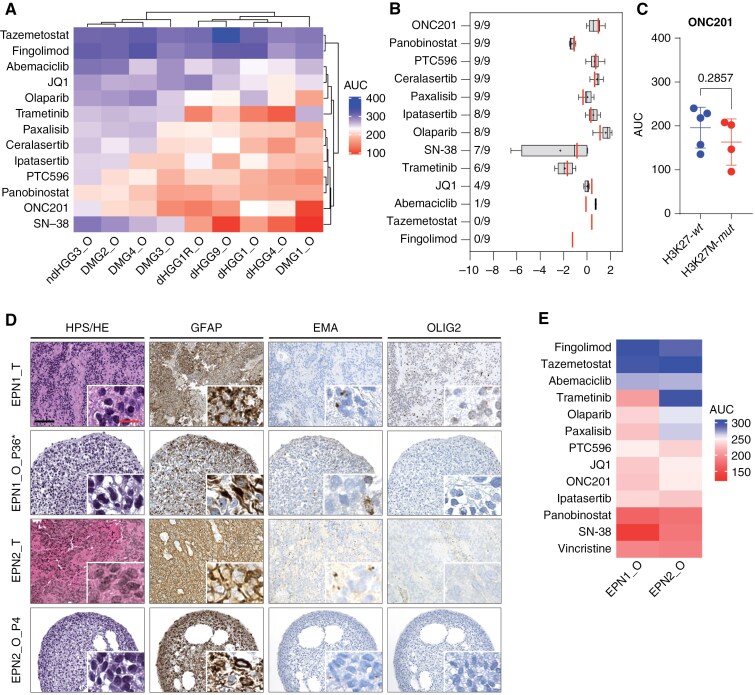
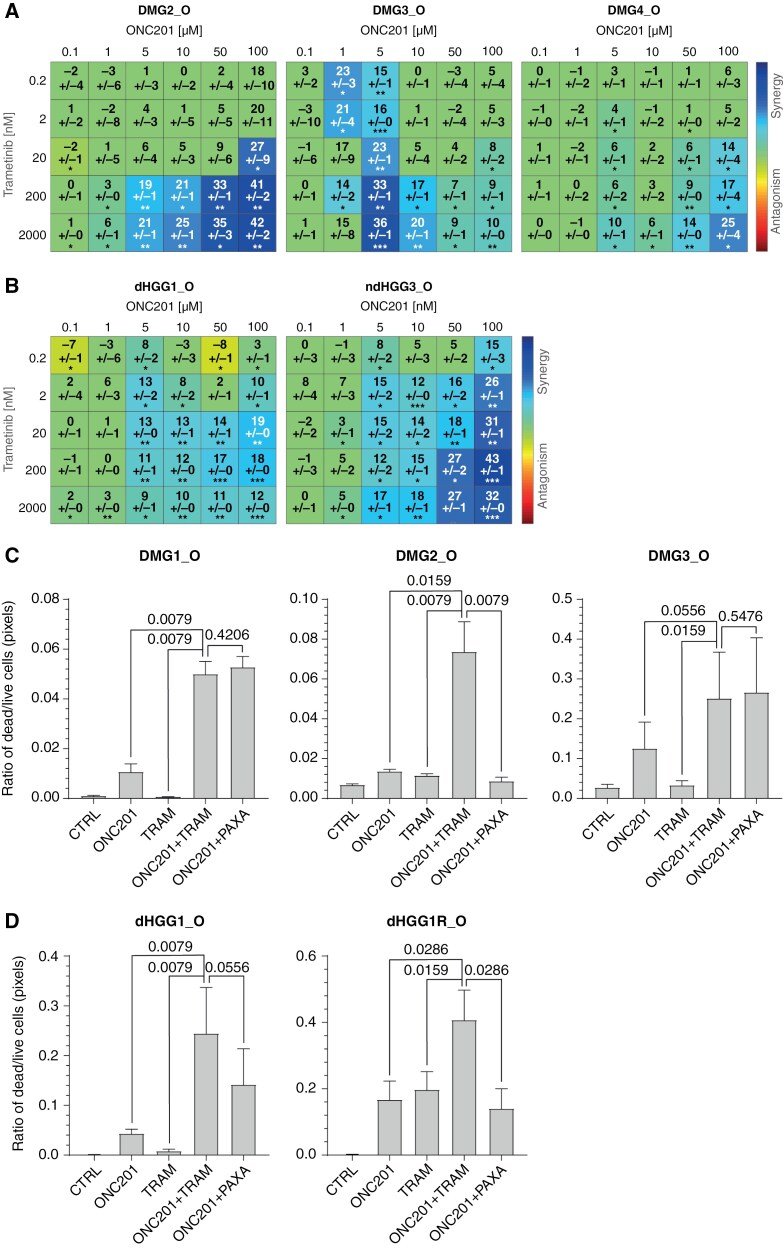
Results: Our methodological pipeline allowed the rapid and efficient generation of PDT-O recapitulating their parental tumor features, including intratumoral heterogeneity, even after several passages and cryopreservation/revival as 3D cultures. Moreover, we successfully performed preclinical test responses on these PDT-O to standard-of-care therapies and new therapeutic options. Finally, we identified ONC201 as a selective drug for pediatric glial tumor types not restricted to H3K27-altered glial tumors, as well as combination strategies to increase the therapeutic response to ONC201.
Conclusions: Hence, we describe a fast and robust process to biobank PDT-O for pediatric glial brain tumors. These PDT-O models have the potential for patient-specific modeling even after long-term expansion in vitro, and we established the proof-of-concept of their usefulness to support powerful preclinical studies.
Keywords: drug combinations; ependymoma; glioma; pediatric brain tumor; tumor organoids.
© The Author(s) 2025. Published by Oxford University Press on behalf of the Society for Neuro-Oncology.
Conflict of interest statement
The authors declare no competing interests.
Figures





References
-
- Pollack IF. Brain tumors in children. N Engl J Med. 1994;331(22):1500–1507. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
