

Healthy Lifestyle Care vs Guideline-Based Care for Low Back Pain: A Randomized Clinical Trial
- PMID: 39792385
- PMCID: PMC11724347
- DOI: 10.1001/jamanetworkopen.2024.53807
Healthy Lifestyle Care vs Guideline-Based Care for Low Back Pain: A Randomized Clinical Trial
Abstract
Importance: An unhealthy lifestyle is believed to increase the development and persistence of low back pain, but there is uncertainty about whether integrating support for lifestyle risks in low back pain management improves patients' outcomes.
Objective: To assess the effectiveness of the Healthy Lifestyle Program (HeLP) compared with guideline-based care for low back pain disability.
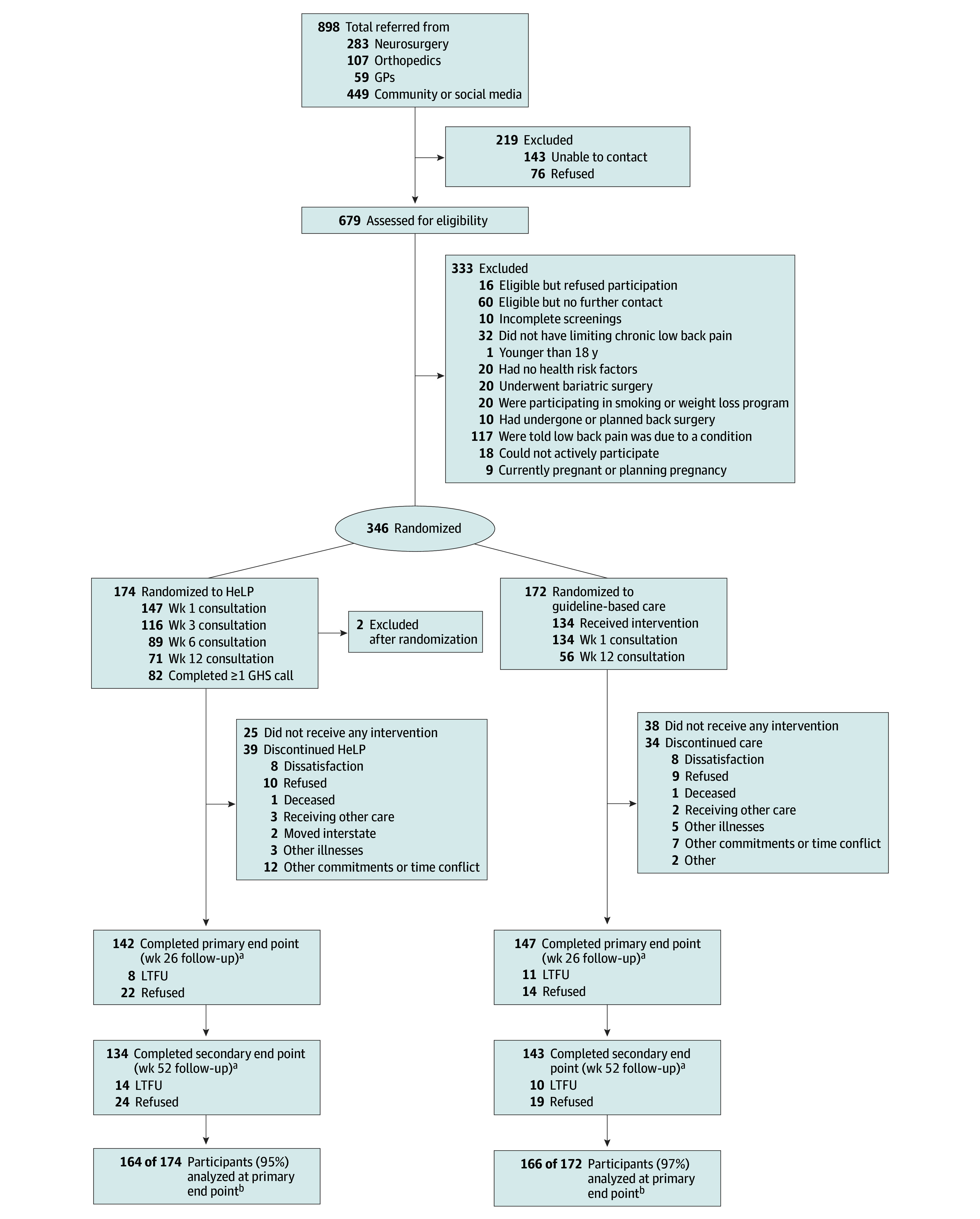
Design, setting, and participants: This superiority, assessor-blinded randomized clinical trial was conducted in Australia from September 8, 2017, to December 30, 2020, among 346 participants who had activity-limiting chronic low back pain and at least 1 lifestyle risk (overweight, poor diet, physical inactivity, and/or smoking), referred from hospital, general practice, and community settings. Statistical analysis was performed from January to December 2021.
Interventions: Participants were block randomized to the HeLP intervention (n = 174; 2 postrandomization exclusions) or guideline-based physiotherapy care (n = 172), stratified by body mass index, using a concealed function in REDCap. HeLP integrated healthy lifestyle support with guideline-based care using physiotherapy and dietetic consultations, educational resources, and telephone-based health coaching over 6 months.
Main outcomes and measures: The primary outcome was low back pain disability (Roland Morris Disability Questionnaire [RMDQ] score; 0-24 scale, where higher scores indicate greater disability) at 26 weeks. Secondary outcomes were weight, pain intensity, quality of life, and smoking. Analyses were performed by intention to treat. We estimated the complier average causal effect (CACE) as sensitivity analyses.
Results: The sample of 346 individuals (mean [SD] age, 50.2 [14.4] years; 190 female participants [55%]) had a baseline mean (SD) RMDQ score of 14.7 (5.4) in the intervention group and 14.0 (5.5) in the control group. At 26 weeks, the between-group difference in disability was -1.3 points (95% CI, -2.5 to -0.2 points; P = .03) favoring HeLP. CACE analysis revealed clinically meaningful benefits in disability among compliers, favoring HeLP (-5.4 points; 95% CI, -9.7 to -1.2 points; P = .01). HeLP participants lost more weight (-1.6 kg; 95% CI, -3.2 to -0.0 kg; P = .049) and had greater improvement in quality of life (physical functioning score; 1.8, 95% CI, 0.1-3.4; P = .04) than control participants.
Conclusions and relevance: Combining healthy lifestyle management with guideline-based care for chronic low back pain led to small improvements in disability, weight, and quality of life compared with guideline-based care alone, without additional harm. Targeting lifestyle risks in the management of chronic low back pain may be considered safe and may offer small additional health benefits beyond current guideline-based care.
Trial registration: http://anzctr.org.au Identifier: ACTRN12617001288314.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
