

Ultrasensitive detection of intact SARS-CoV-2 particles in complex biofluids using microfluidic affinity capture
- PMID: 39792670
- PMCID: PMC11721714
- DOI: 10.1126/sciadv.adh1167
Ultrasensitive detection of intact SARS-CoV-2 particles in complex biofluids using microfluidic affinity capture
Abstract
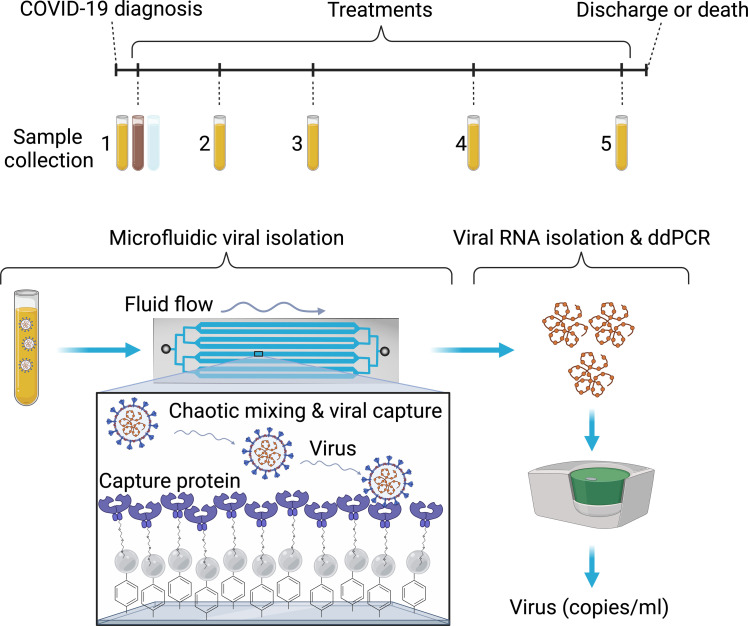
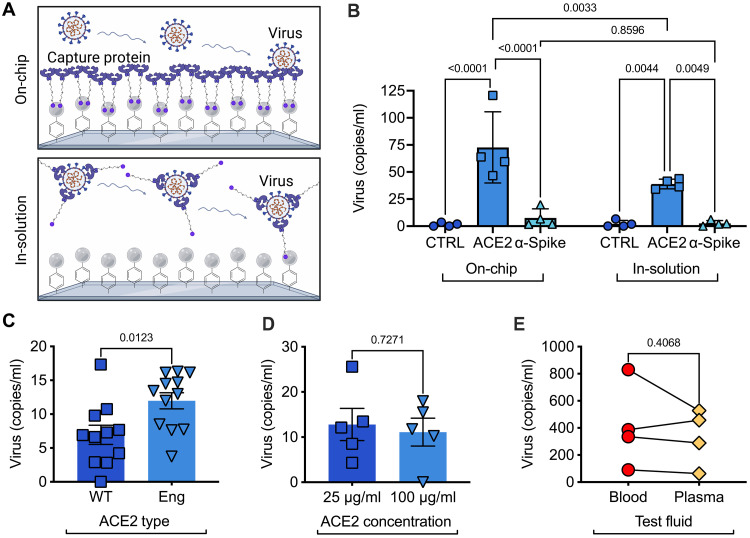
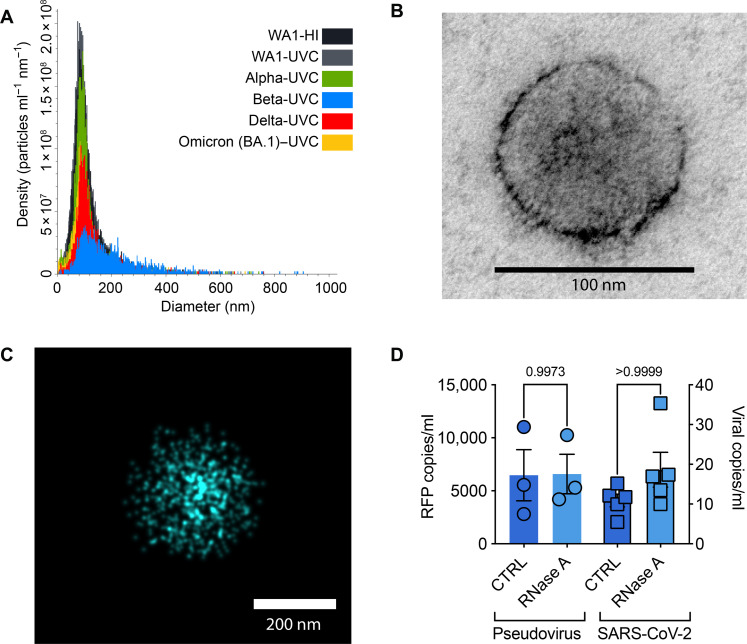
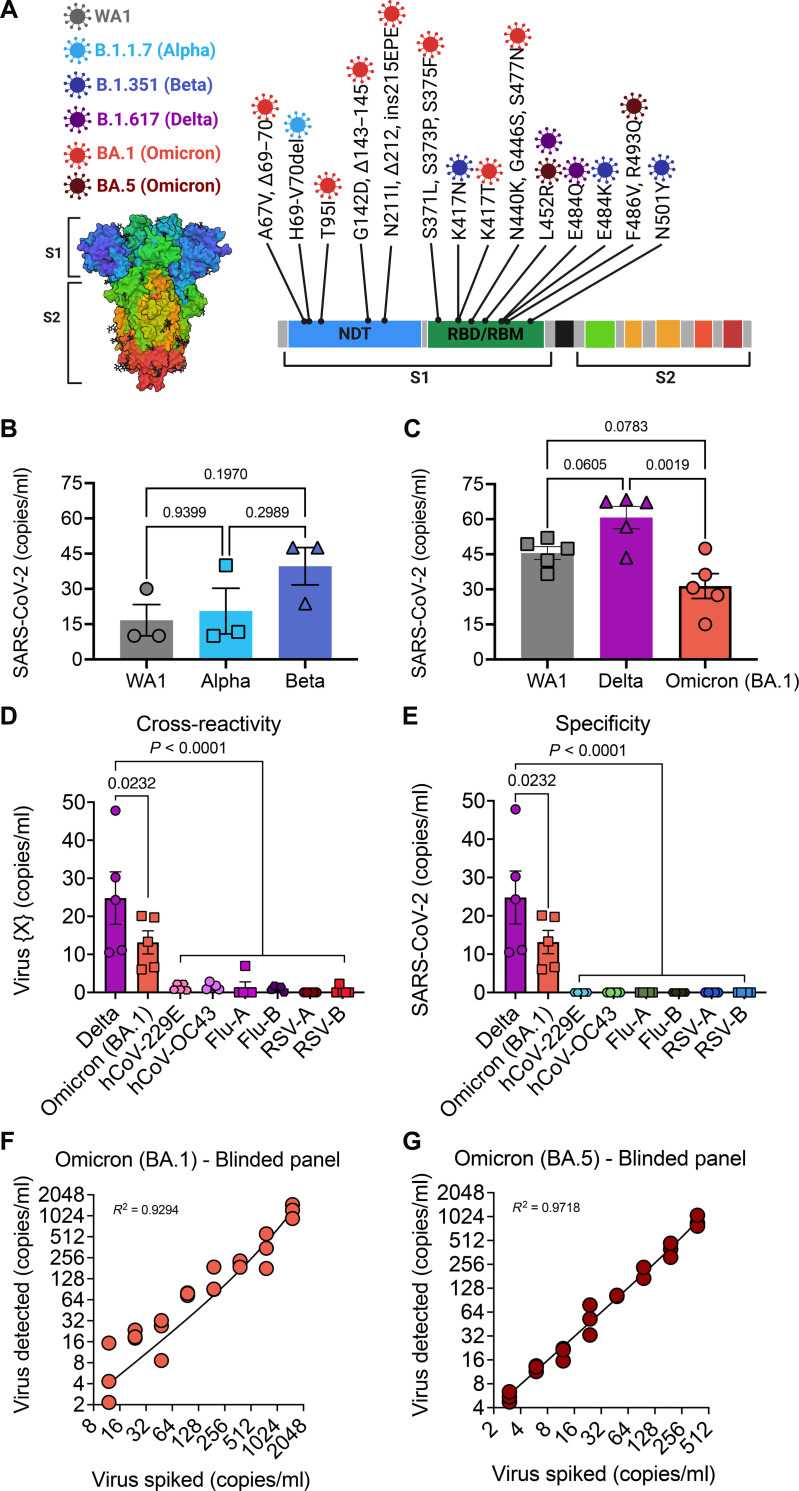
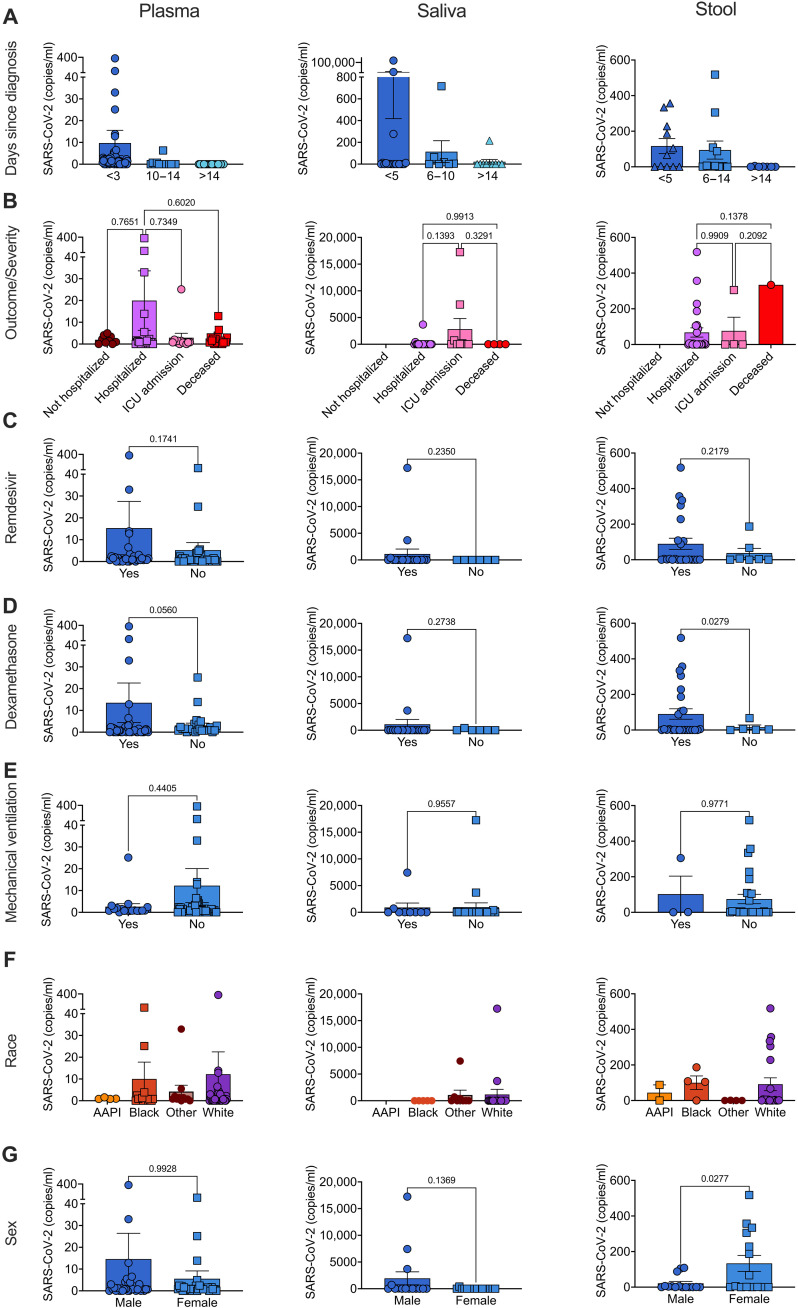
Measuring virus in biofluids is complicated by confounding biomolecules coisolated with viral nucleic acids. To address this, we developed an affinity-based microfluidic device for specific capture of intact severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Our approach used an engineered angiotensin-converting enzyme 2 to capture intact virus from plasma and other complex biofluids. Our device leverages a staggered herringbone pattern, nanoparticle surface coating, and processing conditions to achieve detection of as few as 3 viral copies per milliliter. We further validated our microfluidic assay on 103 plasma, 36 saliva, and 29 stool samples collected from unique patients with COVID-19, showing SARS-CoV-2 detection in 72% of plasma samples. Longitudinal monitoring in the plasma revealed our device's capacity for ultrasensitive detection of active viral infections over time. Our technology can be adapted to target other viruses using relevant cell entry molecules for affinity capture. This versatility underscores the potential for widespread application in viral load monitoring and disease management.
Figures

Similar articles
-
Electrochemical genomagnetic assay for detection of SARS-CoV-2 RNA using a disposable microfluidic platform.Talanta. 2025 Nov 1;294:128186. doi: 10.1016/j.talanta.2025.128186. Epub 2025 Apr 18. Talanta. 2025. PMID: 40262348
-
Development of a portable multi-step microfluidic device for point-of-care nucleic acid diagnostics.Anal Chim Acta. 2025 Jan 22;1336:343518. doi: 10.1016/j.aca.2024.343518. Epub 2024 Dec 5. Anal Chim Acta. 2025. PMID: 39788671
-
A compartmentalization-free microfluidic digital assay for detecting picogram levels of protein analytes.Lab Chip. 2025 Jun 10;25(12):2862-2873. doi: 10.1039/d5lc00103j. Lab Chip. 2025. PMID: 40351019 Free PMC article.
-
[Applications of separation technology in novel coronavirus research, epidemic prevention and detection].Se Pu. 2021 Jul 8;39(7):679-685. doi: 10.3724/SP.J.1123.2021.03022. Se Pu. 2021. PMID: 34227364 Free PMC article. Review. Chinese.
-
The expression of hACE2 receptor protein and its involvement in SARS-CoV-2 entry, pathogenesis, and its application as potential therapeutic target.Tumour Biol. 2021;43(1):177-196. doi: 10.3233/TUB-200084. Tumour Biol. 2021. PMID: 34420993 Review.
Cited by
-
Integrated horizontal convective PCR system for clinical diagnostics.Sci Adv. 2025 Aug 8;11(32):eadx8434. doi: 10.1126/sciadv.adx8434. Epub 2025 Aug 6. Sci Adv. 2025. PMID: 40768581 Free PMC article.
References
-
- Landi F., Carfì A., Benvenuto F., Brandi V., Ciciarello F., Lo Monaco M. R., Martone A. M., Napolitano C., Pagano F., Paglionico A., Petricca L., Rocchi S., Rota E., Salerno A., Tritto M., Gremese E., Bernabei R., Gemelli Against COVID-19 Post-Acute Care Team , Gemelli Against COVID-19 Post-Acute Care Team. Predictive factors for a new positive nasopharyngeal swab among patients recovered from COVID-19. Am. J. Prev. Med. 60, 13–19 (2021). - PMC - PubMed
-
- Piralla A., Ricchi M., Cusi M. G., Prati P., Vicari N., Scarsi G., Gandolfo C., Anichini G., Terrosi C., Percivalle E., Vecchio Nepita E., Bergami F., Tallarita M., Di Martino R., Ferrari A., Rovida F., Lunghi G., Schiavo R., Baldanti F., Residual SARS-CoV-2 RNA in nasal swabs of convalescent COVID-19 patients: Is prolonged quarantine always justified? Int. J. Infect. Dis. 102, 299–302 (2021). - PMC - PubMed
-
- Landi F., Gremese E., Rota E., Carfi’ A., Benvenuto F., Ciciarello F., Monaco M. R. L., Martone A. M., Pagano F., Paglionico A., Petricca L., Rocchi S., Tritto M., Sanguinetti M., Bernabei R., Gemelli Against COVID-19 Post-Acute Care Team , Positive RT-PCR nasopharyngeal swab in patients recovered from COVID-19 disease: When does quarantine really end? J. Infect. 81, e1–e3 (2020). - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
