

Plasma neutrophil gelatinase-associated lipocalin as a single test rule out biomarker for acute kidney injury: A cross-sectional study in patients admitted to the emergency department
- PMID: 39792804
- PMCID: PMC11723545
- DOI: 10.1371/journal.pone.0316897
Plasma neutrophil gelatinase-associated lipocalin as a single test rule out biomarker for acute kidney injury: A cross-sectional study in patients admitted to the emergency department
Abstract
Objectives: Acute kidney injury (AKI) is a syndrome with high mortality and morbidity in part due to delayed recognition based on changes in creatinine. A marker for AKI based on a single measurement is needed and therefore the performance of a single measurement of plasma neutrophil gelatinase-associated lipocalin (pNGAL) to predict AKI in patients admitted to the emergency department was tested.
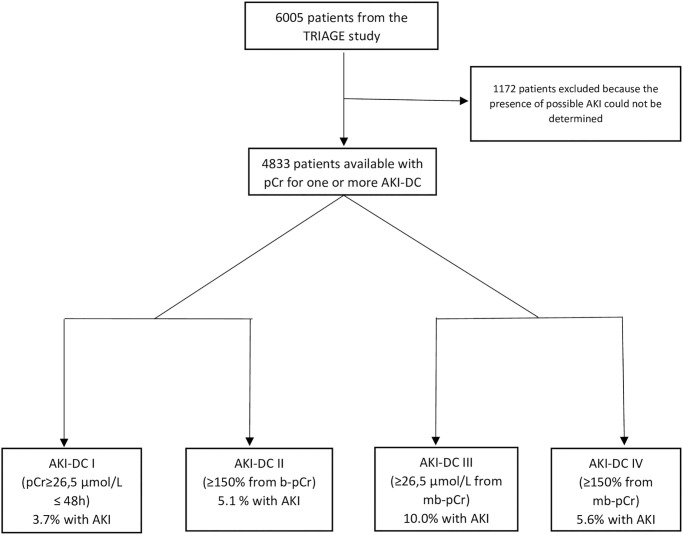
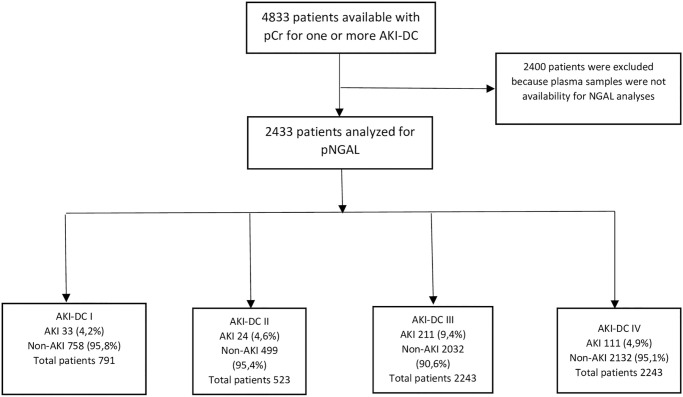
Methods: Samples from the Triage study which included 6005 consecutive adult patients admitted to the emergency department were tested for pNGAL. The optimal cutoff for pNGAL was determined by the AUC and compared to AKI based on creatinine using different estimations of the premorbid kidney function.
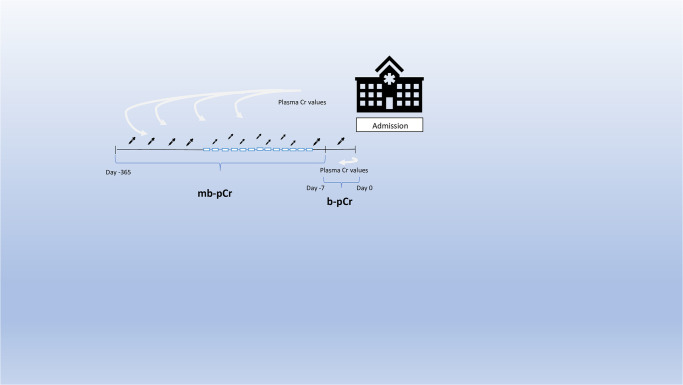
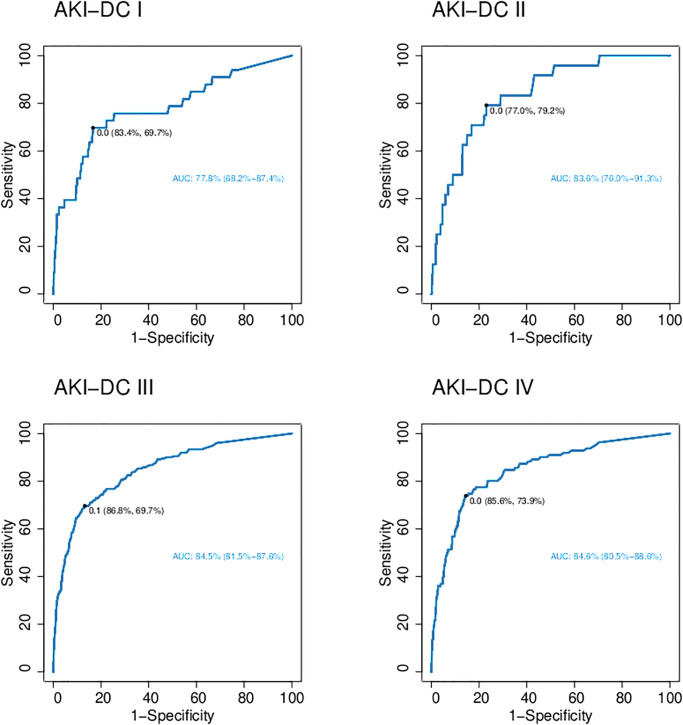
Results: In 4833 patients, two or more plasma creatinine (pCr) measurements were available allowing the detection of AKI. The highest prevalence of AKI (10%) was found when defining AKI as an increase in pCr ≥26.5 μmol/L from the prior year's mean pCr. At these conditions the AUC for pNGAL to predict AKI was 85% giving an optimal cutoff of 142.5 ng/mL with a negative predictive value of 0.96, a positive predictive value of 0.35, a specificity of 0.87 and a sensitivity of 0.70.
Conclusion: The study illustrates that the value of a single measurement of pNGAL is primarily in excluding AKI whereas it`s poorer in predicting the presence of AKI. When diagnosing AKI with pCr the optimal baseline pCr level is the mean of available pCr (mb-pCr) measurements from up to a year prior to the current event.
Copyright: © 2025 Wetterstrand et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Immediate postoperative plasma neutrophil gelatinase-associated lipocalin to predict acute kidney injury after major open abdominal aortic surgery: A prospective observational study.Anaesth Crit Care Pain Med. 2018 Aug;37(4):327-334. doi: 10.1016/j.accpm.2017.09.006. Epub 2017 Oct 12. Anaesth Crit Care Pain Med. 2018. PMID: 29033359
-
Plasma neutrophil gelatinase-associated lipocalin is an early marker of acute kidney injury in adult critically ill patients: a prospective study.J Crit Care. 2010 Mar;25(1):176.e1-6. doi: 10.1016/j.jcrc.2009.05.010. Epub 2009 Sep 24. J Crit Care. 2010. PMID: 19781900
-
Plasma NGAL for the diagnosis of AKI in patients admitted from the emergency department setting.Clin J Am Soc Nephrol. 2013 Dec;8(12):2053-63. doi: 10.2215/CJN.12181212. Epub 2013 Sep 5. Clin J Am Soc Nephrol. 2013. PMID: 24009223 Free PMC article.
-
Neutrophil Gelatinase-Associated Lipocalin Measured on Clinical Laboratory Platforms for the Prediction of Acute Kidney Injury and the Associated Need for Dialysis Therapy: A Systematic Review and Meta-analysis.Am J Kidney Dis. 2020 Dec;76(6):826-841.e1. doi: 10.1053/j.ajkd.2020.05.015. Epub 2020 Jul 15. Am J Kidney Dis. 2020. PMID: 32679151 Free PMC article.
-
Diagnostic value of neutrophil gelatinase-associated lipocalin for early diagnosis of cardiac surgery-associated acute kidney injury: a meta-analysis.Eur J Cardiothorac Surg. 2016 Mar;49(3):746-55. doi: 10.1093/ejcts/ezv199. Epub 2015 Jun 20. Eur J Cardiothorac Surg. 2016. PMID: 26094017 Review.
Cited by
-
Unpacking KDIGO Guidelines: Prioritizing and Applying Exposures and Susceptibilities for AKI in Clinical Practice.J Clin Med. 2025 Apr 9;14(8):2572. doi: 10.3390/jcm14082572. J Clin Med. 2025. PMID: 40283401 Free PMC article.
References
-
- Kellum J. A. et al.., “Kidney disease: Improving global outcomes (KDIGO) acute kidney injury work group. KDIGO clinical practice guideline for acute kidney injury,” Mar. 2012. doi: 10.1038/kisup.2012.1 - DOI
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
