

Evaluation of point-of-care haemoglobin measurement accuracy in surgery (PREMISE) and implications for transfusion practice: a prospective cohort study
- PMID: 39794232
- PMCID: PMC11775836
- DOI: 10.1016/j.bja.2024.09.033
Evaluation of point-of-care haemoglobin measurement accuracy in surgery (PREMISE) and implications for transfusion practice: a prospective cohort study
Abstract
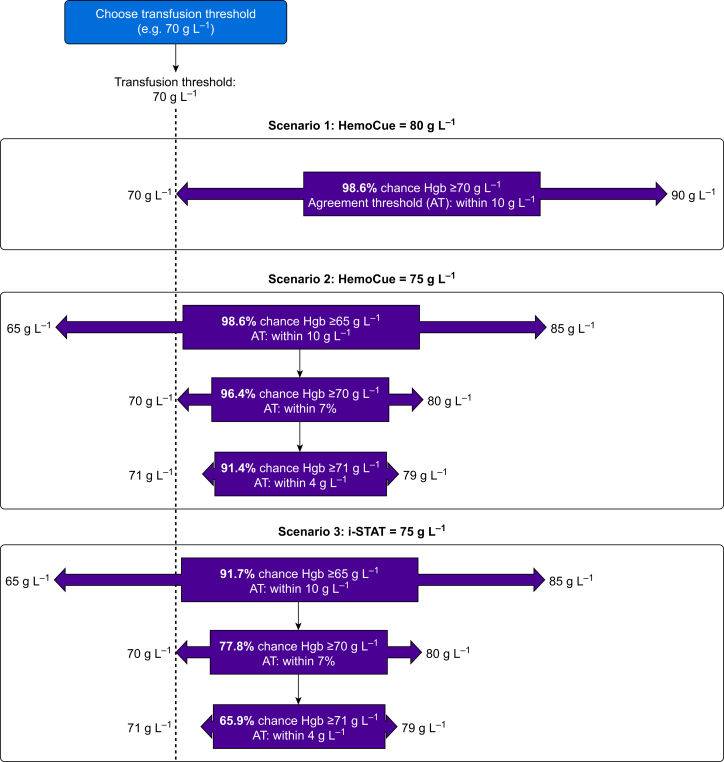
Background: Point-of-care testing devices to measure haemoglobin (Hgb) frequently inform transfusion decision-making in surgery. This study aimed to examine their accuracy in surgery, focusing on Hgb concentrations of 60-100 g L-1, a range with higher potential for transfusion.
Methods: This was a prospective diagnostic cohort study focused on method comparison, conducted at two academic hospitals. Consecutive patients undergoing noncardiac surgery and requiring point-of-care Hgb measurements were eligible. Hgb concentrations from arterial and central venous blood samples were measured concurrently using three devices and compared with laboratory Hgb. The primary outcome was individual pairwise comparisons between point-of-care and laboratory Hgb values; agreement was determined based on a threshold of within 4 g L-1. The primary analysis consisted of computing limits of agreement.
Results: A total of 1735 intraoperative blood samples were collected (1139 participants); 680 samples had a laboratory Hgb <100 g L-1. The limits of agreement among those with Hgb <100 g L-1 were -9.5 to 8.0 g L-1 for HemoCue®, -16.2 to 11.5 g L-1 for i-STAT®, and -14.7 to 40.5 g L-1 for Rad-67®. HemoCue was associated with a 5.8% incidence of potentially clinically significant transfusion error, whereas i-STAT and Rad-67 were associated with 25.3% and 28.2%, respectively. HemoCue yielded Hgb measurements within 10 g L-1 in 98% of intraoperative blood samples.
Conclusions: No point-of-care Hgb device demonstrated limits of agreement that were smaller than the agreement difference of 4 g L-1. Despite this, HemoCue can be safely used to inform transfusion decisions in surgery, given its error probability of <4% in transfusion scenarios.
Keywords: haemoglobin; method comparison; noncardiac surgery; point-of-care; transfusion.
Copyright © 2024 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interest The authors declare that they have no conflict of interest. Specifically, no device manufacturer was involved in funding this study or in any portion of this study.
Figures

References
-
- Whitaker B.I., Rajbhandary S., Harris A. AABB; Bethesda, Maryland: 2015. The 2013 AABB blood collection, utilization, and patient blood management survey report. - PubMed
-
- Callum J., Pinkerton P., Lima A., et al. 4th Edn. ORBCoN; Toronto, ON, Canada: 2016. Bloody easy 4: blood transfusions, blood alternatives and transfusion reactions.
-
- Ackland G.L., Brudney C.S., Cecconi M., et al. Perioperative Quality Initiative consensus statement on the physiology of arterial blood pressure control in perioperative medicine. Br J Anaesth. 2019;122:542–551. - PubMed
-
- Baker L., Park L., Gilbert R., et al. Intraoperative red blood cell transfusion decision-making: a systematic review of guidelines. Ann Surg. 2021;274:86–96. - PubMed
-
- Hutton B., Fergusson D., Tinmouth A., McIntyre L., Kmetic A., Hébert P.C. Transfusion rates vary significantly amongst Canadian medical centres. Can J Anesth. 2005;52:581–590. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
