

Translational and clinical comparison of whole genome and transcriptome to panel sequencing in precision oncology
- PMID: 39794422
- PMCID: PMC11724059
- DOI: 10.1038/s41698-024-00788-3
Translational and clinical comparison of whole genome and transcriptome to panel sequencing in precision oncology
Abstract
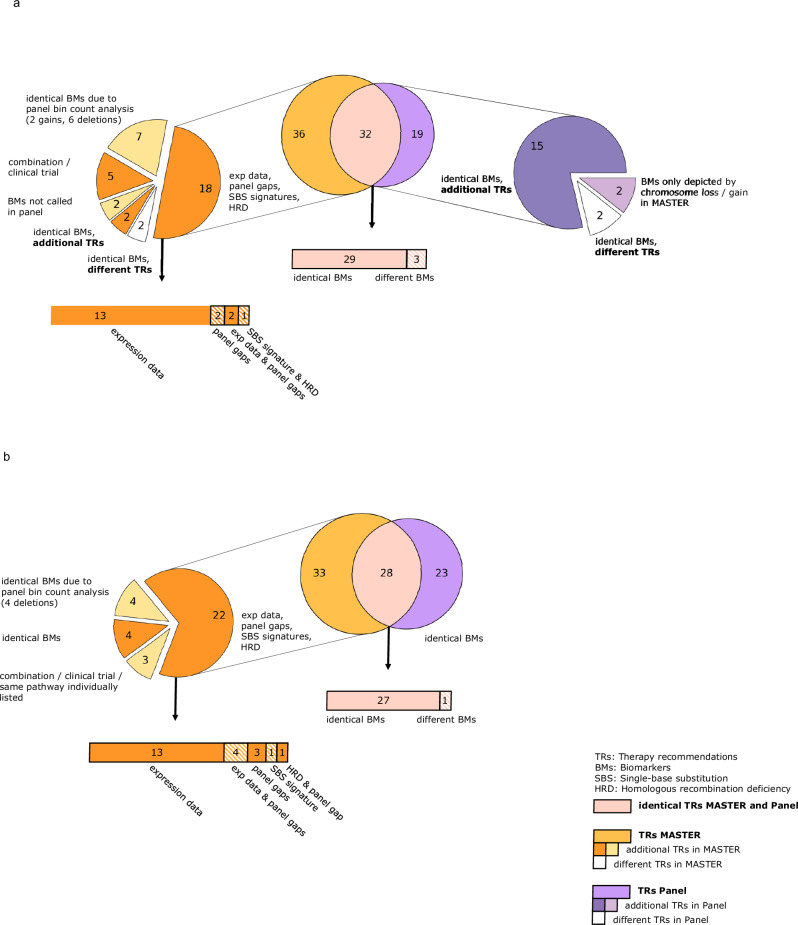
Precision oncology offers new cancer treatment options, yet sequencing methods vary in type and scope. In this study, we compared whole-exome/whole-genome (WES/WGS) and transcriptome sequencing (TS) with broad panel sequencing by resequencing the same tumor DNA and RNA as well as normal tissue DNA for germline assessment, from 20 patients with rare or advanced tumors, who were originally sequenced by WES/WGS ± TS within the DKFZ/NCT/DKTK MASTER program from 2015 to 2020. Molecular analyses resulted in a median number of 2.5 (gene panel) to 3.5 (WES/WGS ± TS) treatment recommendations per patient. Our results showed that approximately half of the therapy recommendations (TRs) of both sequencing programs were identical, while approximately one-third of the TRs in WES/WGS ± TS relied on biomarkers not covered by the panel. Eight of 10 molecularly informed therapy implementations were supported by the panel, the remaining two were based on biomarkers absent from the panel, highlighting the potential additional clinical benefit of WGS and TS.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: I.A.K. reports personal fees from Bayer and stock ownerships in BioNTech, CureVac, Valneva, and Novavax, but declares no non-financial competing interests. C.H. reports honoraria from Novartis and Roche, research funding from Boehringer Ingelheim, and advisory board activities for Boehringer Ingelheim, but declares no non-financial competing interests. L.M. reports financial support from Else Kröner Research College Dresden, a Clinician Scientist Program led by Professor A. El-Armouche, and that his wife is an employee of Pfizer Pharma GmbH, but declares no non-financial competing interests. E.E.M. reports that she became an employee of Pfizer Pharma GmbH after participating in this research project, but declares no non-financial competing interests. M.H. reports personal fees from MSD and stock ownerships in AbbVie, Astellas Pharma, AstraZeneca, Bayer, BridgeBio Pharma, Bristol-Myers Squibb, Daiichi Sankyo, Eisai, Exelixis, Gilead, GSK, Illumina, Incyte, Johnson & Johnson, Merck, MSD, Novartis, Pfizer, PharmaMar, and Roche, but declares no nonfinancial competing interests. The remaining authors declare no competing interests.
Figures



References
-
- Robson, Mark et al. Olaparib for metastatic breast cancer in patients with a germline BRCA mutation. N. Engl. J. Med.377, 523–533 (2017). - PubMed
LinkOut - more resources
Full Text Sources
