

Therapeutic Consequences and Prognostic Impact of Multimorbidity in Heart Failure: Time to Act
- PMID: 39797222
- PMCID: PMC11722306
- DOI: 10.3390/jcm14010139
Therapeutic Consequences and Prognostic Impact of Multimorbidity in Heart Failure: Time to Act
Abstract
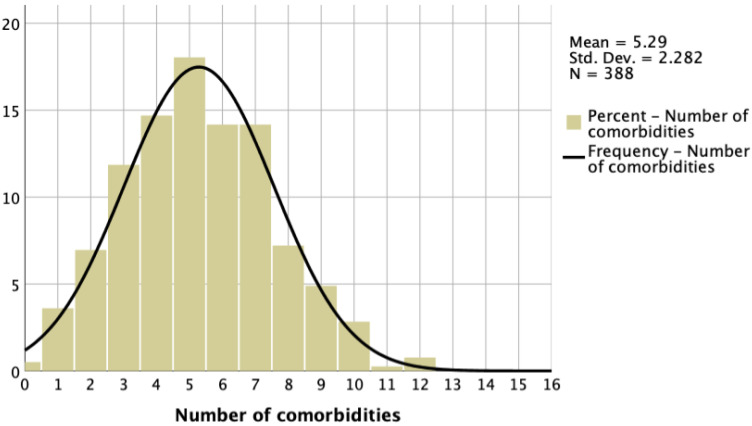
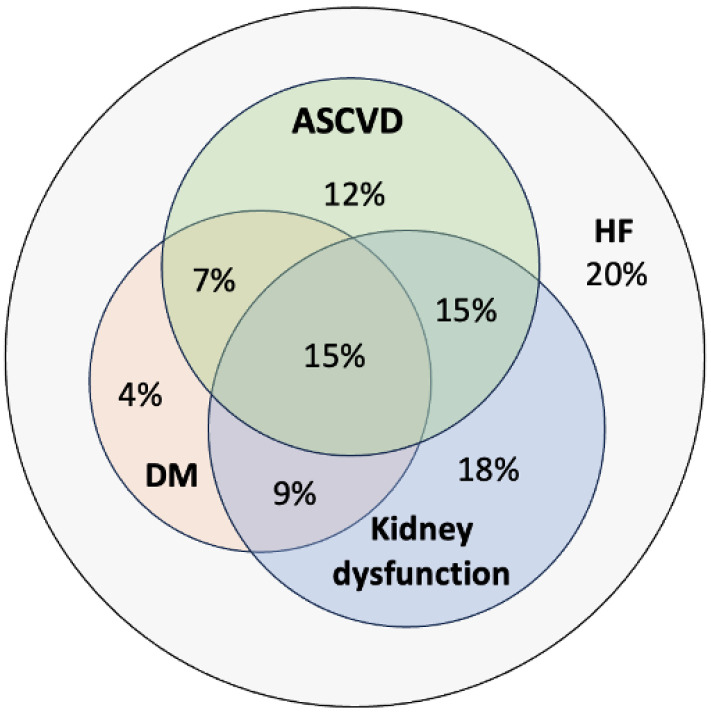
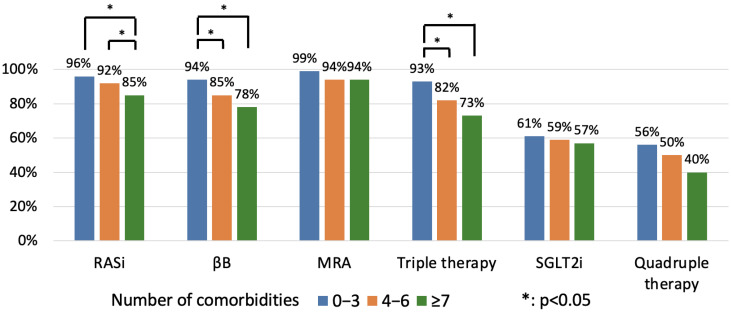
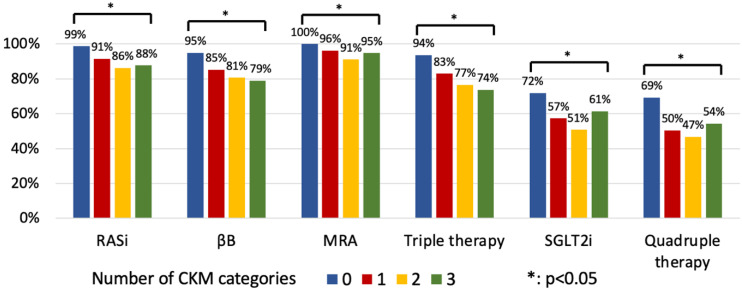
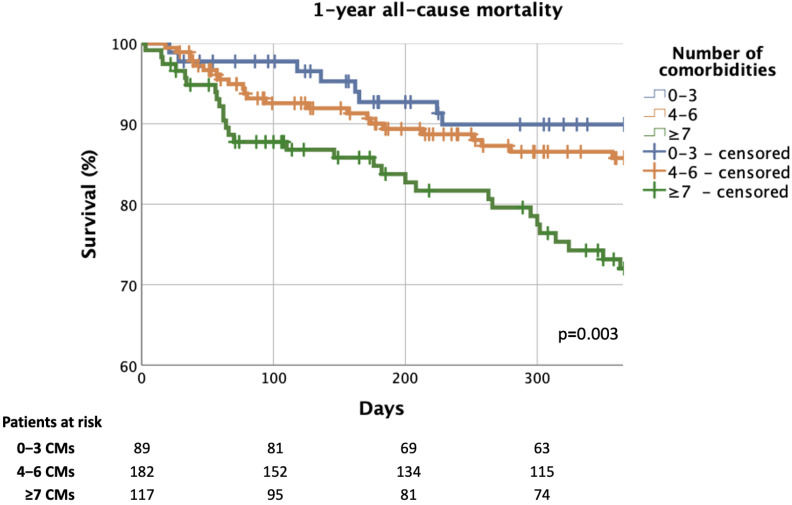
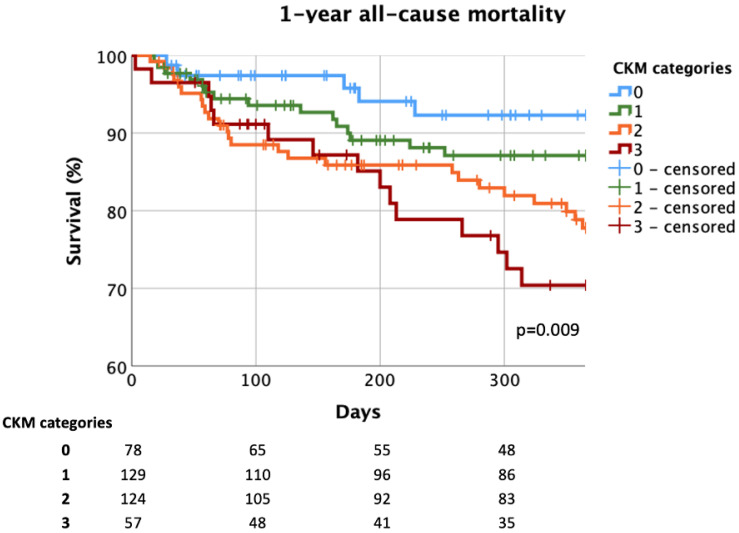
Background/Objectives: In heart failure (HF) with reduced ejection fraction (HFrEF), the early diagnosis and proper treatment of comorbidities (CMs) are of fundamental relevance. Our aim was to assess the prevalence of CMs among real-world patients requiring hospitalisation for HFrEF and to investigate the effect of CMs on the implementation of guideline-directed medical therapy (GDMT) and on all-cause mortality (ACM). Methods: The data of a consecutive HFrEF patient cohort hospitalised for HF between 2021 and 2024 were analysed retrospectively. Sixteen CMs (6 CV and 10 non-CV) were considered. Patients were divided into three categories: 0-3 vs. 4-6 vs. ≥7 CMs. GDMT at discharge and ACM were compared among CM categories. The predictors of 1-year ACM were also evaluated. Results: From the 388 patients (male: 76%, age: 61 [50-70] years; NT-proBNP: 5286 [2570-9923] pg/mL; ≥2 cardiovascular-kidney-metabolic disease overlap: 46%), a large proportion received GDMT (RASi: 91%; βB: 85%; MRA: 95%; SGLT2i: 59%; triple therapy [TT: RASi+βB+MRA]: 82%; quadruple therapy [QT: TT + SGLT2i]: 54%) at discharge. Multimorbidity was accompanied with a (p < 0.05) lower application ratio of RASi (96% vs. 92% vs. 85%; 0-3 vs. 4-6 vs. ≥7 CMs) and βB therapy (94% vs. 85% vs. 78%), while MRA (99% vs. 94% vs. 94%) and SGTL2i use (61% vs. 59% vs. 57%) did not differ (p > 0.05). Patients with multimorbidity were less likely to be treated with TT (93% vs. 82% vs. 73%, p = 0.001), while no difference was detected in the implementation of QT (56% vs. 54% vs. 50%, p = 0.685). The 1-year ACM of patients with an increased burden of CMs was higher (9% vs. 13% vs. 25%, p = 0.003). The risk of 1-year ACM was favourably affected by the use of TT/QT and less severe left ventricular systolic dysfunction, while having ≥5 CMs had an unfavourable impact on prognosis. Conclusions: According to our real-world analysis, HFrEF patients with an increased burden of CMs can expect a less favourable outcome. However, modern GDMT can even be applied in this patient population, resulting in a significantly improved prognosis. Thus, clinicians should insist on the early, conscious implementation of a prognosis-modifying drug regime in multimorbid HF patients as well.
Keywords: comorbidity; guideline-directed medical therapy; heart failure; multimorbidity; prognosis.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Bhatt A.S., Ambrosy A.P., Dunning A., DeVore A.D., Butler J., Reed S., Voors A., Starling R., Armstrong P.W., Ezekowitz J.A., et al. The burden of non-cardiac comorbidities and association with clinical outcomes in an acute heart failure trial—Insights from ASCEND-HF. Eur. J. Heart Fail. 2020;22:1022–1031. doi: 10.1002/ejhf.1795. - DOI - PMC - PubMed
-
- Tomasoni D., Vitale C., Guidetti F., Benson L., Braunschweig F., Dahlström U., Melin M., Rosano G.M.C., Lund L.H., Metra M., et al. The role of multimorbidity in patients with heart failure across the left ventricular ejection fraction spectrum: Data from the Swedish Heart Failure Registry. Eur. J. Heart Fail. 2024;26:854–868. doi: 10.1002/ejhf.3112. - DOI - PubMed
-
- Conrad N., Judge A., Tran J., Mohseni H., Hedgecott D., Crespillo A.P., Allison M., Hemingway H., Cleland J.G., McMurray J.J.V., et al. Temporal trends and patterns in heart failure incidence: A population-based study of 4 million individuals. Lancet. 2018;391:572–580. doi: 10.1016/S0140-6736(17)32520-5. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
