

Correlation between in vivo imaging and post‑mortem autopsy findings for the medico-legal evaluation of a right hepatic artery pseudoaneurysm as a fatal complication of laparoscopic cholecystectomy
- PMID: 39797962
- PMCID: PMC12325457
- DOI: 10.1007/s12024-024-00937-x
Correlation between in vivo imaging and post‑mortem autopsy findings for the medico-legal evaluation of a right hepatic artery pseudoaneurysm as a fatal complication of laparoscopic cholecystectomy
Abstract
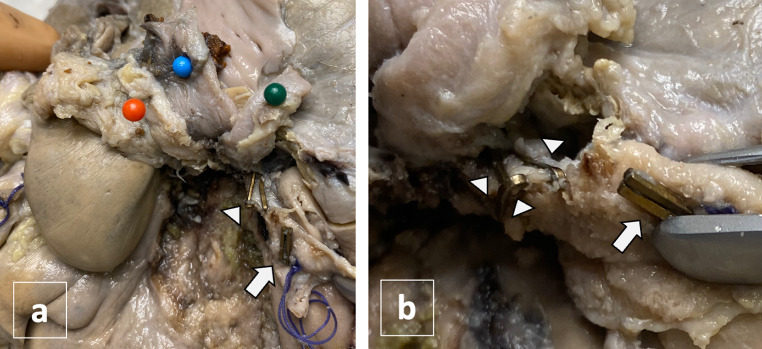
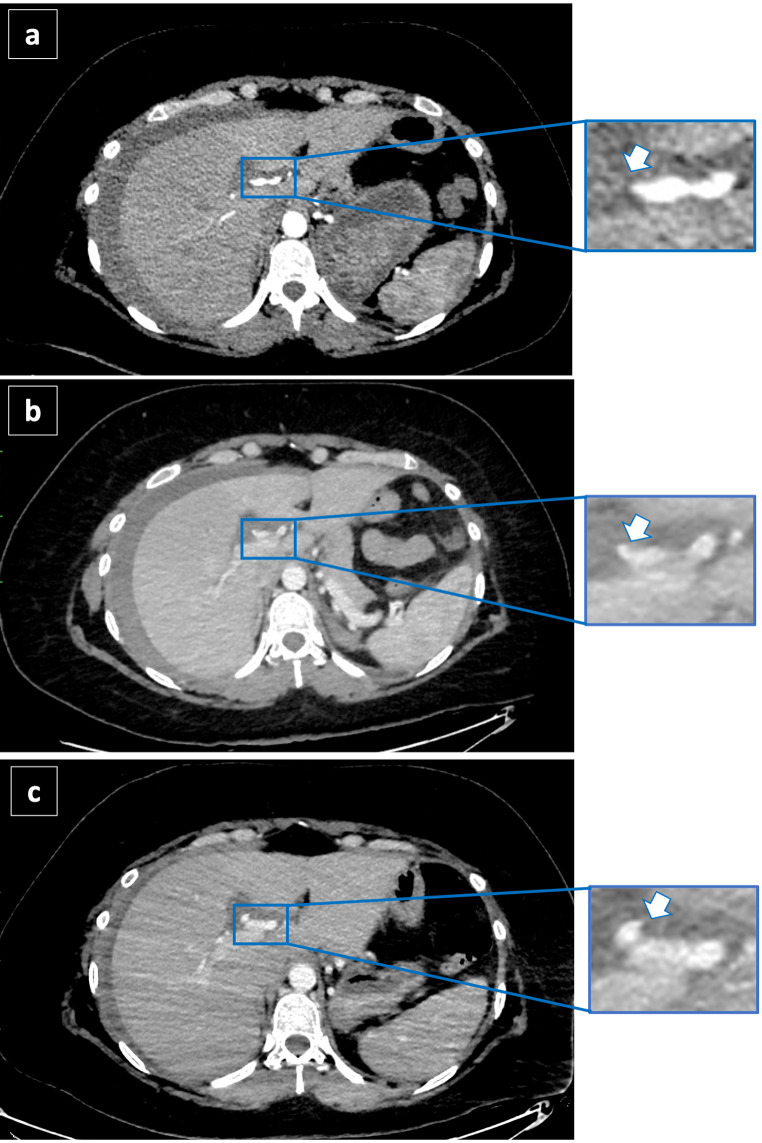
A 36-year-old woman diagnosed with complicated cholecystolithiasis underwent elective laparoscopic cholecystectomy (LC), then converted to open cholecystectomy because of a massive intraoperative bleeding. Hemostasis was performed with clipping and suturing the source of bleeding. In post-operative period, the patient suffered from persistent anemia associated with hemoperitoneum diagnosed through abdominal CT scanning, in absence of any sign of active bleeding. She died 16 days after the surgical procedure. Autopsy revealed the presence of 2 clips adjacent to the suture used for ligating the cystic artery and the presence of 3 surgical metal clips on the right hepatic artery, that should not be present in a routine cholecystectomy. The review of CT scans performed during the hospital stay revealed contrast extravasation from the right hepatic artery, near the 3 clips, allowing the post-mortem diagnosis of pseudoaneurysm (PA). The diagnosis of PA of right hepatic artery is typically made in living patients, through imaging, and autoptic identification is rarely obtained. The innovation of this report is to present an iconographic correlation between in vivo imaging and autopsy data, allowing for the tracing of the PA's origin to the wall weakening caused by the placement of 3 clips on the right hepatic artery, and having significant medico-legal implications.
Keywords: Autopsy; Cholecystectomy; Intraoperative bleeding; Post-mortem CT; Right hepatic artery pseudoaneurysm.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: N/A. Ethics approval and consent to participate: The current Italian legislation neither requires the family’s consent or ethical approval for a single case, as long as the data are kept strictly anonymous. Because summoning the parents was not possible as it would badly interfere with the grieving process, parents’ consent was waived, according to the Italian Authority of Privacy and Data Protection (“Garante della Privacy”: GDPR nr 679/2016; 9/2016 and recent law addition number 424/ 19th of July 2018; http://www.garanteprivacy . it). Competing interests: None.
Figures
References
-
- Nicholson T, Travis S, Ettles D, Dyet J, Sedman P, Wedgewood K, Royston C. Hepatic artery angiography and embolization for hemobilia following laparoscopic cholecystectomy. Cardiovasc Intervent Radiol. 1999 Jan. - PubMed
-
- Saad NE, Saad WE, Davies MG, Waldman DL, Fultz PJ, Rubens DJ. Pseudoaneurysms and the role of minimally invasive techniques in their management. Radiographics. 2005. - PubMed
-
- Belfonte C, Sanderson A, Dejenie F. Quincke’s triad: a rare complication of a common outpatient procedure. Am J Gastroenterol. 2011;106:S277.
-
- Caminiti R, Rossitto M, Ciccolo A. (2011) Pseudoaneurysm of the hepatic artery and Hemobilia: a rare complication of laparoscopic cholecystectomy; clinical case and literature review. Acta Chir Belg, 111. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
