

Durvalumab with or without bevacizumab with transarterial chemoembolisation in hepatocellular carcinoma (EMERALD-1): a multiregional, randomised, double-blind, placebo-controlled, phase 3 study
- PMID: 39798579
- PMCID: PMC12282661
- DOI: 10.1016/S0140-6736(24)02551-0
Durvalumab with or without bevacizumab with transarterial chemoembolisation in hepatocellular carcinoma (EMERALD-1): a multiregional, randomised, double-blind, placebo-controlled, phase 3 study
Abstract
Background: Transarterial chemoembolisation (TACE) is standard of care for patients with unresectable hepatocellular carcinoma that is amenable to embolisation; however, median progression-free survival is still approximately 7 months. We aimed to assess whether adding durvalumab, with or without bevacizumab, might improve progression-free survival.
Methods: In this multiregional, randomised, double-blind, placebo-controlled, phase 3 study (EMERALD-1), adults aged 18 years or older with unresectable hepatocellular carcinoma amenable to embolisation, an Eastern Cooperative Oncology Group performance status of 0 or 1 at enrolment, and at least one measurable intrahepatic lesion per modified Response Evaluation Criteria in Solid Tumours (RECIST) were enrolled at 157 medical sites including research centres and general and specialist hospitals in 18 countries. Eligible patients were randomly assigned (1:1:1), stratified by TACE method, region, and portal vein invasion, using an interactive voice response or web response system, to TACE plus either durvalumab plus bevacizumab (1500 mg intravenous durvalumab once every 4 weeks, then 1120 mg durvalumab plus 15 mg/kg intravenous bevacizumab once every 3 weeks), durvalumab plus placebo (same regimen using placebo instead of bevacizumab), or placebo alone (same regimen using placebo instead of durvalumab and instead of bevacizumab). Participants, investigators, and those assessing outcomes were masked to treatment assignment until data analysis. The primary endpoint was progression-free survival, by blinded independent central review (BICR), and per RECIST version 1.1, with durvalumab plus bevacizumab versus placebo alone in the intention-to-treat population (ITT; ie, all participants assigned to treatment). Key secondary endpoints were progression-free survival by BICR per RECIST version 1.1 with durvalumab plus placebo versus placebo alone, overall survival, and time to deterioration in select patient-reported outcomes. Participants continue to be followed up for overall survival, and overall survival and patient-reported outcomes will be reported in a later publication. Safety was assessed in the safety analysis set, which included all participants assigned to treatment who received any study treatment (ie, any durvalumab, bevacizumab, or placebo) by treatment received. This study is registered with ClinicalTrials.gov, NCT03778957, and is closed to accrual.
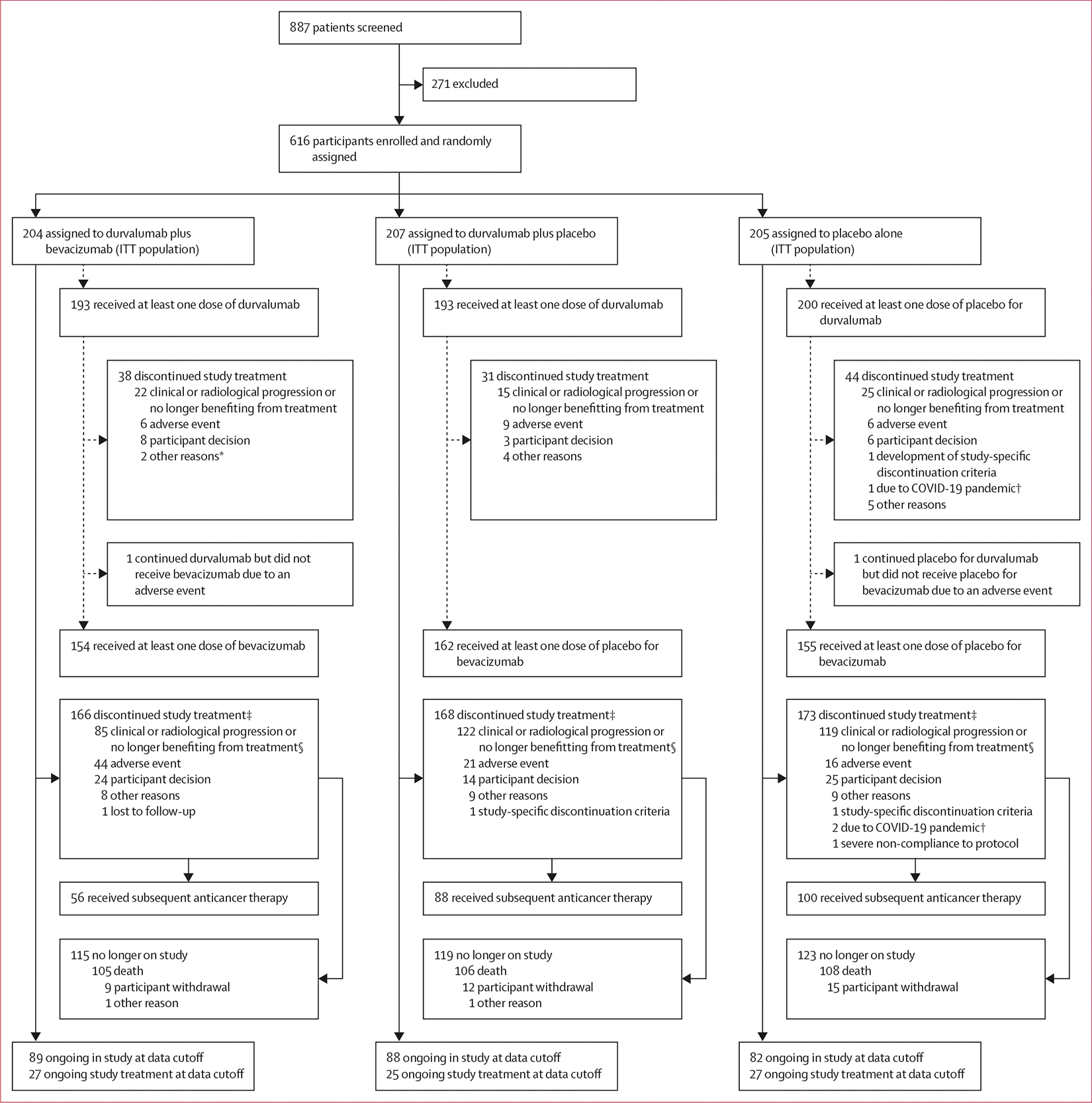
Findings: Between Nov 30, 2018, and July 19, 2021, 887 patients were screened, of whom 616 were randomly assigned to durvalumab plus bevacizumab (n=204), durvalumab plus placebo (n=207), or placebo alone (n=205; ITT population). Median age was 65·0 years (IQR 59·0-72·0), 135 (22%) of 616 participants were female, 481 (78%) were male, 375 (61%) were Asian, 176 (29%) were White, 22 (4%) were American Indian or Alaska Native, nine (1%) were Black or African American, one (<1%) was native Hawaiian or other Pacific Islander, and 33 (5%) were other races. As of data cutoff (Sept 11, 2023) median follow-up for progression-free survival was 27·9 months (95% CI 27·4-30·4), median progression-free survival was 15·0 months (95% CI 11·1-18·9) with durvalumab plus bevacizumab, 10·0 months (9·0-12·7) with durvalumab, and 8·2 months (6·9-11·1) with placebo. Progression-free survival hazard ratio was 0·77 (95% CI 0·61-0·98; two-sided p=0·032) for durvalumab plus bevacizumab versus placebo, and 0·94 (0·75-1·19; two-sided p=0·64) for durvalumab plus placebo versus placebo. The most common maximum grade 3-4 adverse events were hypertension in participants who received durvalumab and bevacizumab (nine [6%] of 154 participants), anaemia in participants who received durvalumab and placebo (ten [4%] of 232 participants), and post-embolisation syndrome in participants who received placebo alone (eight [4%] of 200 participants). Study treatment-related adverse events that led to death occurred in none of 154 participants who received durvalumab and bevacizumab, three (1%) of 232 who received durvalumab and placebo (n=1 for arterial haemorrhage, liver injury, and multiple organ dysfunction syndrome), and three (2%) of 200 who received placebo alone (n=1 for oesophageal varices haemorrhage, upper gastrointestinal haemorrhage, and dermatomyositis).
Interpretation: Durvalumab plus bevacizumab plus TACE has the potential to set a new standard of care. With additional follow-up of the EMERALD-1 study, future analyses, including the final overall survival data and patient-reported outcomes, will help to further characterise the potential clinical benefits of durvalumab plus bevacizumab plus TACE in hepatocellular carcinoma amenable to embolisation.
Funding: AstraZeneca.
Copyright © 2025 Elsevier Ltd. All rights reserved, including those for text and data mining, AI training, and similar technologies.
Conflict of interest statement
Declaration of interests BS reports consultancy fees from AstraZeneca, Bristol Myers Squibb, Eisai, GlaxoSmithKline, Merck Sharp & Dohme, Roche, and Sanofi; payment or honoraria from AstraZeneca, Eisai, Roche, and Sirtex Medical; and support for travel or attending meetings from AstraZeneca and Roche. MK reports grants or contracts from AbbVie, Chugai Pharmaceutical, Eisai, GE HealthCare Japan, Otsuka Pharmaceutical, and Taiho Pharmaceutical; consultancy fees from AstraZeneca, Chugai Pharmaceutical, Eisai, and Roche; and payment or honoraria from AstraZeneca, Chugai Pharmaceutical, Eisai, Eli Lilly, and Takeda. JPE reports consultancy fees from AstraZeneca and fees for participation on a data safety monitoring board or advisory board from AstraZeneca. ZR reports consultancy fees from AstraZeneca, Merck Sharp & Dohme, and Roche; and fees for participation on a data safety monitoring board or advisory board from AstraZeneca, Merck Sharp & Dohme, and Roche. SLC reports grants or contracts from Celleron, Genorbio, Ipsen, Merck Sharp & Dohme, Novartis, and Sirtex Medical; consultancy fees from AstraZeneca, Autem Therapeutics, Eisai, and Merck Sharp & Dohme; payment or honoraria from AstraZeneca, Bayer, Bristol Myers Squibb, Eisai, Hutchison MediPharma, Ipsen, Merck Sharp & Dohme, and Roche; and support for travel or attending meetings from AstraZeneca, Eisai, Ipsen, and Roche. YA reports payment or honoraria from AstraZeneca and fees for participation on a data safety monitoring board or advisory board from AstraZeneca. JH reports grants or contracts from Roche; consultancy fees from AbbVie Korea, GlaxoSmithKline, and Immunocore; payment or honoraria from AstraZeneca, Gilead Sciences, Oncolys BioPharma, Roche, and Yuhan Korea; and leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid, from AstraZeneca. JE reports grants or contracts from AstraZeneca, Bristol Myers Squibb, and Merck Sharp & Dohme; payment or honoraria from Asofarma Pharma; support for travel or attending meetings from Astellas Pharma, AstraZeneca, Bristol Myers Squibb, Janssen, Merck Sharp & Dohme and Roche; and being a board member for Sociedad Mexicana de Oncología. J-HY reports grants or contracts from Dicerna Pharmaceuticals, GlaxoSmithKline, Mediver, Merck Sharp & Dohme, NewG-Lab Pharma, Pharmicell, Roche, and Vir Biotechnology. VVB reports consultancy fees, payment or honoraria, and fees for participation on a data safety monitoring board or advisory board from AstraZeneca, Bayer, Eisai, and Roche. TS reports payment or honoraria from American Taiwan Biopharm, AstraZeneca (Thailand), Berlin Pharmaceutical Industry, DKSH (Thailand), Janssen, Reckitt Benckiser (Thailand), Roche Thailand, Roche Diagnostics (Thailand), Sandoz (Thailand), Takeda (Thailand), and Thai Otsuka Pharmaceutical; and support for travel or attending meetings from American Taiwan Biopharm, AstraZeneca (Thailand), Berlin Pharmaceutical Industry, DKSH (Thailand), Ferring Pharmaceuticals, Reckitt Benckiser (Thailand), Roche Thailand, Roche Diagnostics (Thailand), Takeda (Thailand), and Thai Meiji. MB reports consultancy fees from AbbVie, AstraZeneca, Bayer, Bristol Myers Squibb, Eisai, Merck Sharp & Dohme, Roche, Sirtex Medical, and Taiho Pharmaceutical; and payment or honoraria from Bayer and Sirtex Medical. S-ML reports honoraria from Roche; support for travel or attending meetings from AstraZeneca and Roche; fees for participation on an advisory board from AstraZeneca; and an unpaid position as President and Honoured President of the Taiwan Liver Cancer Association. J-MP reports grants or contracts, consultancy fees, payment or honoraria, and support for travel or attending meetings from AbbVie, Bayer, Gilead Sciences, Ipsen, and Roche. C-FC reports grants or contracts from AbbVie, Aceta Pharma, AstraZeneca, Bayer, Bristol Meyers Squibb, Genentech, Translational Research In Oncology, and Roche; payment or honoraria from Roche; fees for participation on a data safety monitoring board or advisory board from Roche; and a role as an expert on the Committee of National Health Insurance Administration (Taiwan). MM reports support for travel or attending meetings from AstraZeneca. MŻ is an employee of AstraZeneca. SIU and GJC are employees of AstraZeneca and hold stock in AstraZeneca. JFK is an employee of AstraZeneca; holds stock in AstraZeneca; reports support for travel or attending meetings from ASCO Breakthrough; and is listed as co-inventor with MedImmune as the applicant on patents PCT/US2018/018513 (WO2018/152415), filed Feb 16, 2018, and with AstraZeneca as the applicant on patents PCT/EP2021/062695 (WO2021/228978), filed May 12, 2021, and PCT/EP2022/079828 (2023/174569), filed Oct 25, 2022. RL reports consultancy fees from AstraZeneca. All other authors declare no competing interests.
Figures



Comment in
-
TACE plus immune checkpoint inhibitor-based systemic therapies for hepatocellular carcinoma.Lancet. 2025 Jan 18;405(10474):174-176. doi: 10.1016/S0140-6736(24)02680-1. Epub 2025 Jan 8. Lancet. 2025. PMID: 39798580 No abstract available.
-
Durvalumab and bevacizumab plus transarterial chemoembolization in unresectable hepatocellular carcinoma: a new paradigm?Transl Gastroenterol Hepatol. 2026 Jan 22;11:1. doi: 10.21037/tgh-25-34. eCollection 2026. Transl Gastroenterol Hepatol. 2026. PMID: 41675315 Free PMC article. No abstract available.
References
-
- Vogel A, Cervantes A, Chau I, et al. Hepatocellular carcinoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol 2018; 29 (suppl 4): iv238–55. - PubMed
-
- Llovet JM, Bruix J. Systematic review of randomized trials for unresectable hepatocellular carcinoma: chemoembolization improves survival. Hepatology 2003; 37: 429–42. - PubMed
-
- Bolondi L, Burroughs A, Dufour J-F, et al. Heterogeneity of patients with intermediate (BCLC B) hepatocellular carcinoma: proposal for a subclassification to facilitate treatment decisions. Semin Liver Dis 2012; 32: 348–59. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
