

The effectiveness of two doses of recombinant hepatitis E vaccine in response to an outbreak in Bentiu, South Sudan: a case-control and bias indicator study
- PMID: 39798583
- PMCID: PMC12018298
- DOI: 10.1016/S1473-3099(24)00657-1
The effectiveness of two doses of recombinant hepatitis E vaccine in response to an outbreak in Bentiu, South Sudan: a case-control and bias indicator study
Abstract
Background: Hepatitis E virus (HEV) is a leading cause of acute viral hepatitis, particularly in Asia and Africa, where HEV genotypes 1 and 2 are prevalent. Although a recombinant vaccine, Hecolin, is available, it has not been used to control outbreaks. The licensed three-dose regimen might pose challenges for it to be an impactful outbreak control tool. Our study aimed to estimate the effectiveness of two doses of Hecolin in the context of the first-ever reactive use of the vaccine.
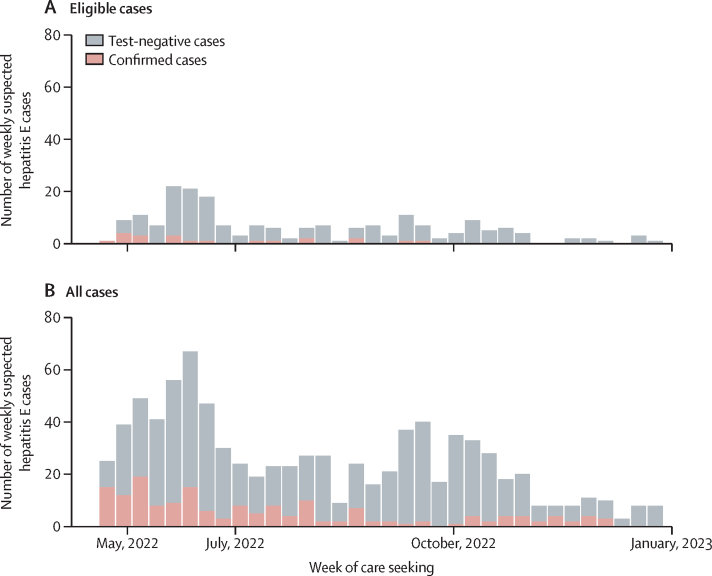
Methods: We conducted a case-control study during an HEV outbreak in the Bentiu internally displaced persons camp, South Sudan. Patients with acute jaundice syndrome (suspected cases) seeking care at the Médecins Sans Frontières hospital were screened for study eligibility. Eligible participants were those that had been eligible for vaccination (ie, living in the camp and aged 16-40 years). Confirmed cases were defined as individuals who tested positive for hepatitis E by RT-PCR or anti-HEV IgM ELISA. Each case was matched to six controls by age, sex, pregnancy status, and residence. Self-reported vaccination status was verified through vaccination cards. The primary analysis was two-dose vaccine effectiveness, which we estimated with a matched case-control design using conditional logistic regression models. In secondary analyses we estimated vaccine effectiveness using a test-negative design and the screening method. We used test-negative cases and their matched controls as a bias indicator analysis to help quantify potential health seeking behaviour biases.
Findings: Between May 10 and Dec 30, 2022, we identified 859 patients with suspected hepatitis E. Of these, 201 met the eligibility criteria and 21 cases had laboratory confirmed hepatitis E. Among the confirmed cases, 10 (48%) were unvaccinated compared with 33 (27%) of 121 matched controls. In the primary analysis we estimated an unadjusted two-dose vaccine effectiveness of 67·8% (95% CI -28·6 to 91·9), and a two-dose vaccine effectiveness of 84·0% (-208·5 to 99·2) after adjustment for potential confounders. The bias indicator analysis suggested that test-negative cases might have been more likely to have been vaccinated than their matched community controls due to different health-care seeking behaviours, potentially meaning underestimation of effectiveness estimates. The test-negative design, which uses facility-matched controls, led to an adjusted two-dose effectiveness of 89·4% (56·4 to 98·0).
Interpretation: Despite the small sample size, our estimates provide evidence of effectiveness of a two-dose regimen against HEV genotype 1 during a protracted outbreak, supporting its use in similar contexts.
Funding: Médecins Sans Frontières.
Copyright © 2025 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests MSF provided support in the form of salaries for ASA, VKA, PGi, PN, JD, MH, PGa, MA, MR, and IC and indirectly provided salary support for Epicentre employees RCN and EG. ASA serves as a member of the Gavi, the Vaccine Alliance Independent Review Committee. All other authors declare no competing interests.
Figures

References
-
- Kamar N, Izopet J, Pavio N, et al. Hepatitis E virus infection. Nat Rev Dis Primers. 2017;3 - PubMed
-
- Rein DB, Stevens GA, Theaker J, Wittenborn JS, Wiersma ST. The global burden of hepatitis E virus genotypes 1 and 2 in 2005. Hepatology. 2012;55:988–997. - PubMed
-
- Bergløv A, Hallager S, Weis N. Hepatitis E during pregnancy: maternal and foetal case-fatality rates and adverse outcomes-a systematic review. J Viral Hepat. 2019;26:1240–1248. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
