

Associations of daily step count with all-cause mortality and cardiovascular mortality in hypertensive US adults: a cohort study from NHANES 2005-2006
- PMID: 39799282
- PMCID: PMC11725191
- DOI: 10.1186/s12889-024-21216-y
Associations of daily step count with all-cause mortality and cardiovascular mortality in hypertensive US adults: a cohort study from NHANES 2005-2006
Abstract
Background: The health benefits of physical activity, including walking, are well-established, but the relationship between daily step count and mortality in hypertensive populations remains underexplored. This study investigates the association between daily step count and both all-cause and cardiovascular mortality in hypertensive American adults.
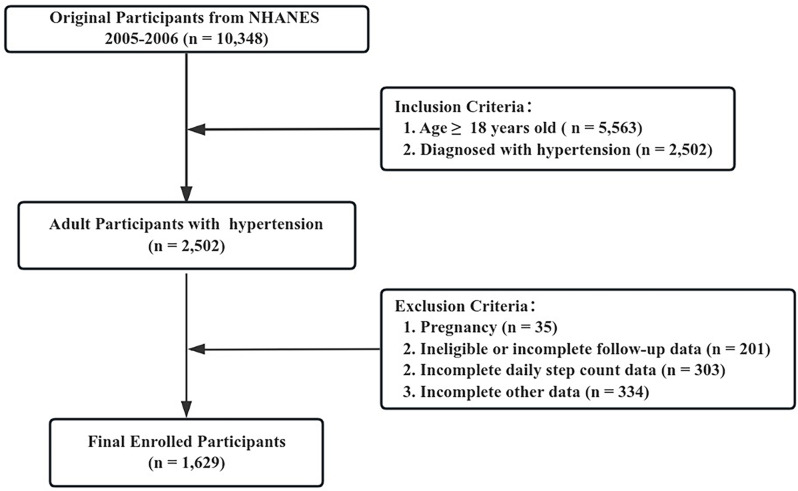
Methods: We used data from the National Health and Nutrition Examination Survey 2005-2006, including 1,629 hypertensive participants with accelerometer-measured step counts. Cox proportional hazards models and restricted cubic spline regression were employed to assess the associations between daily step count and mortality outcomes. Analyses were adjusted for demographics, lifestyle factors, and comorbidities.
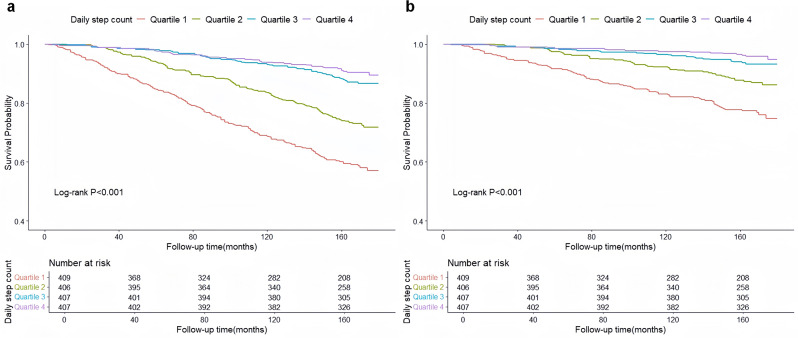
Results: Over an average follow-up of 12.57 years, 370 deaths occurred, of which 177 were due to cardiovascular causes. We observed non-linear associations between daily step count and mortality. Mortality risks were significantly reduced with step counts to 8,250 steps/day for all-cause mortality and 9,700 steps/day for cardiovascular mortality. Beyond these thresholds, the benefits plateaued.
Conclusion: Increasing daily step count is associated with reduced all-cause and cardiovascular mortality in hypertensive individuals, with optimal benefits observed below 8,250 and 9,700 daily steps, respectively. Moderate levels of physical activity provide substantial health benefits, highlighting the importance of setting realistic and attainable activity goals for hypertensive populations.
Keywords: Daily step count; Hypertension; Mortality; NHANES.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The ethics review board of the National Center for Health Statistics approved all NHANES protocols, and written informed consents were obtained from all participants or their proxies. All the experiment protocol for involving humans was in accordance to guidelines of national/international/institutional or Declaration of Helsinki in the manuscript. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures


References
-
- Martin SS, Aday AW, Almarzooq ZI, Anderson CAM, Arora P, Avery CL, Baker-Smith CM, Barone Gibbs B, Beaton AZ, Boehme AK, et al. 2024 Heart Disease and Stroke statistics: a report of US and Global Data from the American Heart Association. Circulation. 2024;149(8):e347–913. - PubMed
-
- Heidenreich PA, Trogdon JG, Khavjou OA, Butler J, Dracup K, Ezekowitz MD, Finkelstein EA, Hong Y, Johnston SC, Khera A, et al. Forecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart Association. Circulation. 2011;123(8):933–44. - PubMed
-
- Pelliccia A, Sharma S, Gati S, Bäck M, Börjesson M, Caselli S, Collet JP, Corrado D, Drezner JA, Halle M, et al. 2020 ESC guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur Heart J. 2021;42(1):17–96. - PubMed
-
- Liu X, Zhang D, Liu Y, Sun X, Han C, Wang B, Ren Y, Zhou J, Zhao Y, Shi Y, et al. Dose-response Association between Physical Activity and Incident Hypertension: a systematic review and Meta-analysis of Cohort studies. Hypertension. 2017;69(5):813–20. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
