

The association between self-reported total gestational weight gain by pre-pregnancy body mass index and moderate to late preterm birth
- PMID: 39799301
- PMCID: PMC11724485
- DOI: 10.1186/s12884-024-07106-6
The association between self-reported total gestational weight gain by pre-pregnancy body mass index and moderate to late preterm birth
Abstract
Background: Inadequate and excessive gestational weight gain (GWG) defined by the Institute of Medicine (IOM) has been associated with preterm birth. However, studies demonstrate inconsistent associations.
Objectives: We examined the associations between categorical and continuous total GWG and moderate to late preterm birth (32-<37 weeks), and evaluated differences in these associations by pre-pregnancy BMI.
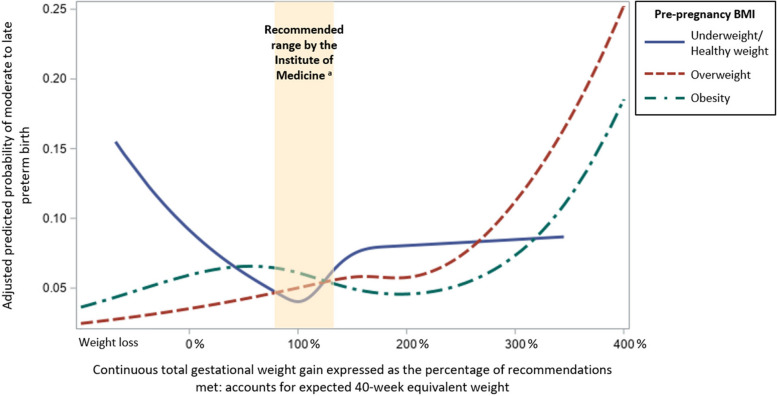
Methods: We analyzed cross-sectional data from children participating in TARGet Kids! in Toronto, Canada. Parents of children < 6 years of age recalled pre-pregnancy weight, end-of-pregnancy weight, and gestational age. GWG was categorized according to the 2009 IOM guidelines as inadequate, recommended, or excessive for each pre-pregnancy BMI category. GWG was expressed as the percentage of recommendations met to account for gestational duration. Adjusted odds ratios (aORs) for moderate to late preterm birth were estimated using logistic regression models. Restricted cubic splines were used to model the adjusted predicted probability of moderate to late preterm birth against continuous GWG.
Results: Of the 4,529 participants, 8.2% were born moderate to late preterm. 31.1% of parents met the GWG recommendations, 41.0% had excessive GWG, and 27.9% had inadequate GWG. Compared to recommended GWG, excessive GWG had increased odds of moderate to late preterm birth (aOR 1.68, 95% CI 1.29, 2.19). There was insufficient evidence of an association between inadequate GWG and moderate to late preterm birth (aOR 1.10, 95% CI 0.81, 1.50). For parents who were overweight or had obesity, the risk of moderate to late preterm birth did not increase substantially until a GWG > 200% of the recommendations, which is well above the IOM recommended upper limit.
Conclusions: Excessive GWG was associated with an increased risk of moderate to late preterm birth, with variation in the association by pre-pregnancy BMI. Current definitions of excessive GWG may not adequately reflect increased risk of preterm birth among those with overweight or obesity.
Keywords: Body mass index; Gestational weight gain; Pregnancy; Premature birth.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Ethics approval was provided by Clinical Trials Ontario with the board of record as the Research Ethics Board at The Hospital for Sick Children (#2063). Informed, written consent was obtained from parents/caregivers of all participating children. TARGet Kids! adhered to the Declaration of Helsinki. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures


References
-
- Institute of Medicine (US) Committee on Understanding Premature Birth and Assuring Healthy Outcomes. Preterm Birth: Causes, Consequences, and Prevention. (Behrman RE, Butler AS, eds.). National Academies Press (US). 2007. Accessed August 15, 2022. http://www.ncbi.nlm.nih.gov/books/NBK11362/. - PubMed
-
- Canadian Institute for Health Information. Hospitalization and childbirth, 1995–1996 to 2021–2022 — supplementary statistics. Ottawa, ON: CIHI; 2023. https://www.cihi.ca/sites/default/files/document/hospital-childbirth-199....
-
- Health Canada. Canadian Perinatal Health Report, 2000. Ottawa: Minister of Public Works and Government Services Canada; 2000. https://publications.gc.ca/collections/Collection/H49-142-2000E.pdf.
-
- Public Health Agency of Canada. Canadian Perinatal Health Report, 2008 Edition. Ottawa; 2008. https://www.phac-aspc.gc.ca/publicat/2008/cphr-rspc/pdf/cphr-rspc08-eng.pdf.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
