

Cognitive Behavioural Therapy to Optimize Post-Operative Recovery (COPE): a randomized controlled feasibility trial in extremity fracture patients
- PMID: 39799376
- PMCID: PMC11724510
- DOI: 10.1186/s40814-024-01592-3
Cognitive Behavioural Therapy to Optimize Post-Operative Recovery (COPE): a randomized controlled feasibility trial in extremity fracture patients
Abstract
Background: Outcomes following surgery to operatively manage extremity fractures are variable, and up to two-thirds of patients report chronic post-surgical pain. Preliminary evidence suggests that psychotherapy directed at improving coping skills and reducing somatic vigilance may improve outcomes among fracture patients. The objective of this pilot study was to test the feasibility and acceptability of a randomized controlled trial comparing an online cognitive behavioural therapy (CBT) program versus usual care in patients with an operatively managed open or closed extremity fracture.
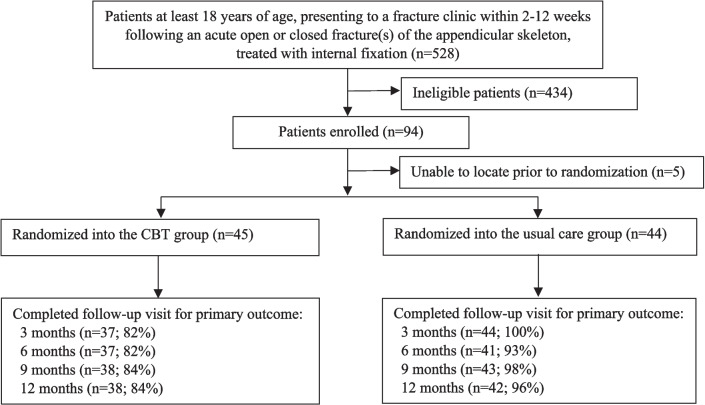
Methods: We conducted a single-centre internal pilot study over a 10-month period in patients with at least one operatively managed open or closed fracture of the appendicular skeleton. Participants were randomized to an online CBT program or usual care and followed for 12 months. The goals of our pilot study were to determine an acceptable rate of recruitment, the degree to which participants randomized to CBT were compliant with treatment, the site investigator's ability to adhere to study protocol and data collection procedures, and our ability to achieve high follow-up rates. Feasibility criteria were evaluated using a graded "traffic light" approach, in which "green light" indicates moving forward with the definitive trial, "yellow light" indicates proceeding with modifications to the protocol and trial procedures, and "red light" indicates a definitive trial is not feasible without significant protocol and trial procedure modifications.
Results: We enrolled 94 participants over 10 months, which resulted in a "yellow light" for recruitment. Participant compliance with completion of the online CBT program received a "yellow light", with 60% of participants who were randomized to CBT completing all seven modules. However, 40% of participants in the CBT-arm withdrew from the program, resulting in a "red light". Adherence with the study protocol activities at baseline was relatively high (88%) which resulted in a "yellow light". Follow-up was 85% (80 of 94) at 12 months, resulting in a "yellow light".
Conclusions: These results suggest feasibility of a definitive, multi-centre trial to compare CBT versus usual care in the management of persistent post-operative pain in fracture patients despite the pilot phase identifying some challenges with enrollment timelines, compliance with the CBT program, and participant follow-up. For the definitive trial, we will expand participant recruitment to additional centres and implement strategies to optimize participant engagement and compliance with the CBT program and follow-up.
Trial registration: ClincialTrials.gov (NCT04274530). Registered February 18, 2020, https://classic.
Clinicaltrials: gov/ct2/show/NCT04274530 .
Keywords: Chronic pain; Cognitive behavioural therapy; Feasibility; Pilot study.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The trial was approved by the Hamilton Integrated Research Ethics Board (#4336) and by all participating clinical sites’ research ethics boards/institutional review boards. Informed consent was obtained from every enrolled participant. Consent for publication: Not applicable. Competing interests: SS reports editorial or governing board for BMC Women’s Health, employment from Global Research Solutions Inc., and employment from McMaster University, outside the submitted work. HJ reports paid presenter or speaker for DePuy, A Johnson & Johnson Company, and board or committee member for the Orthopaedic Research Society, outside the submitted work. JWB is supported, in part, by a Canadian Institutes of Health Research Canada Research Chair in the prevention and management of chronic pain. All other authors have nothing to disclose.
References
-
- Busse JW, Heels-Ansdell D, Makosso-Kallyth S, et al. Patient coping and expectations predict recovery after major orthopaedic trauma. Br J Anaesth. 2019;122(1):51–9. 10.1016/j.bja.2018.06.021. - PubMed
-
- Katsoulis E, Court-Brown C, Giannoudis PV. Incidence and aetiology of anterior knee pain after intramedullary nailing of the femur and tibia. J Bone Joint Surg Br. 2006;88(5):576–80. - PubMed
-
- Linton SJ. A review of psychological risk factors in back and neck pain. Spine (Phila Pa 1976). 2000;25(9):1148–56. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
