

Integration of clinical, pathological, radiological, and transcriptomic data improves prediction for first-line immunotherapy outcome in metastatic non-small cell lung cancer
- PMID: 39800784
- PMCID: PMC11725576
- DOI: 10.1038/s41467-025-55847-5
Integration of clinical, pathological, radiological, and transcriptomic data improves prediction for first-line immunotherapy outcome in metastatic non-small cell lung cancer
Abstract
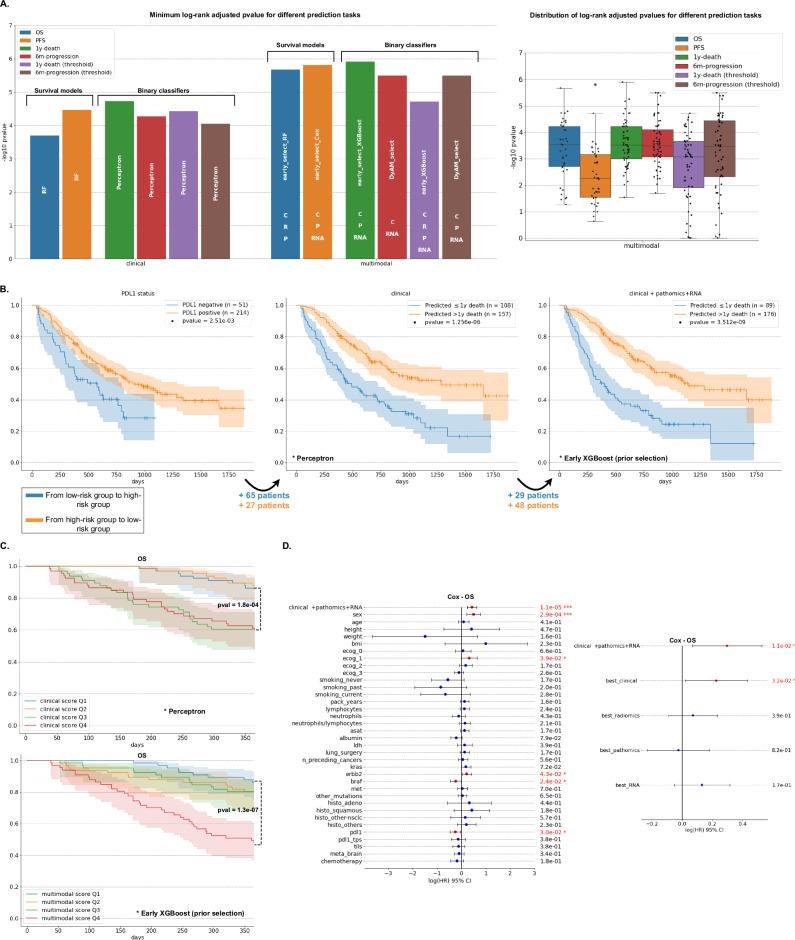
Immunotherapy is improving the survival of patients with metastatic non-small cell lung cancer (NSCLC), yet reliable biomarkers are needed to identify responders prospectively and optimize patient care. In this study, we explore the benefits of multimodal approaches to predict immunotherapy outcome using multiple machine learning algorithms and integration strategies. We analyze baseline multimodal data from a cohort of 317 metastatic NSCLC patients treated with first-line immunotherapy, including positron emission tomography images, digitized pathological slides, bulk transcriptomic profiles, and clinical information. Testing multiple integration strategies, most of them yield multimodal models surpassing both the best unimodal models and established univariate biomarkers, such as PD-L1 expression. Additionally, several multimodal combinations demonstrate improved patient risk stratification compared to models built with routine clinical features only. Our study thus provides evidence of the superiority of multimodal over unimodal approaches, advocating for the collection of large multimodal NSCLC datasets to develop and validate robust and powerful immunotherapy biomarkers.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: Nicolas Girard has a consulting or advisory role for the following companies: Abbvie, AMGEN, AstraZeneca, BeiGene, Bristol-Myers Squibb, Daiichi Sankyo/Astra Zeneca, Gilead Sciences, Ipsen, Janssen, LEO Pharma, Lilly, MSD, Novartis, Pfizer, Roche, Sanofi, Takeda. The other authors declare no competing interests.
Figures







References
-
- Hendriks, L. E. et al. Non-oncogene-addicted metastatic non-small-cell lung cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol.34, 358–376 (2023). - PubMed
-
- Reck, M. et al. Updated analysis of KEYNOTE-024: Pembrolizumab versus platinum-based chemotherapy for advanced non-small-cell lung cancer with PD-L1 tumor proportion score of 50% or greater. J. Clin. Oncol.37, 537–546 (2019). - PubMed
-
- Gandhi, L. et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N. Engl. J. Med.378, 2078–2092 (2018). - PubMed
-
- Paz-Ares, L. et al. A randomized, placebo-controlled trial of pembrolizumab plus chemotherapy in patients with metastatic squamous NSCLC: Protocol-specified final analysis of KEYNOTE-407. J. Thorac. Oncol.15, 1657–1669 (2020). - PubMed
-
- Herbst, R. S. et al. Atezolizumab for first-line treatment of PD-L1-selected patients with NSCLC. N. Engl. J. Med.383, 1328–1339 (2020). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
