

Prevention and Management of Posterior Wound Complications Following Oncologic Spine Surgery: Narrative Review of Available Evidence and Proposed Clinical Decision-Making Algorithm
- PMID: 39801119
- PMCID: PMC11726526
- DOI: 10.1177/21925682241237486
Prevention and Management of Posterior Wound Complications Following Oncologic Spine Surgery: Narrative Review of Available Evidence and Proposed Clinical Decision-Making Algorithm
Erratum in
-
Corrigenda, 2025.Global Spine J. 2025 Jun 11:21925682251343890. doi: 10.1177/21925682251343890. Online ahead of print. Global Spine J. 2025. PMID: 40500909 Free PMC article. No abstract available.
Abstract
Study design: Narrative Review.
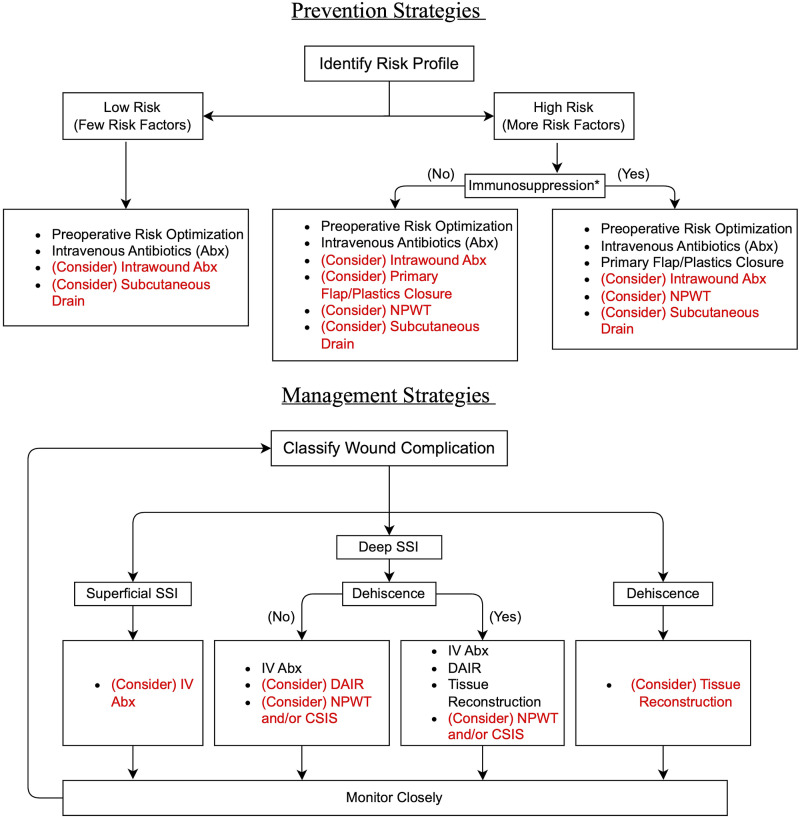
Objective: Contextualized by a narrative review of recent literature, we propose a wound complication prevention and management algorithm for spinal oncology patients. We highlight available strategies and motivate future research to identify optimal and individualized wound management for this population.
Methods: We conducted a search of recent studies (2010-2022) using relevant keywords to identify primary literature in support of current strategies for wound complication prevention and management following spine tumor surgery. When primary literature specific to spine tumor cases was not available, data were extrapolated from studies of other spine surgery populations. Results were compiled into a proposed clinical algorithm to guide practice considering available evidence.
Results: Based on available literature, we recommend individualized stratification of patients according to identifiable risk factors for wound complication and propose several interventions which might be employed preventatively, including intrawound antibiotic administration, negative pressure wound therapy, and primary flap closure of the surgical wound. Of these, the available evidence, weighing possible risks vs benefits, most strongly favors primary flap closure of surgical wounds, particularly for patients with multiple risk factors. A secondary algorithm to guide management of wound complications is also proposed.
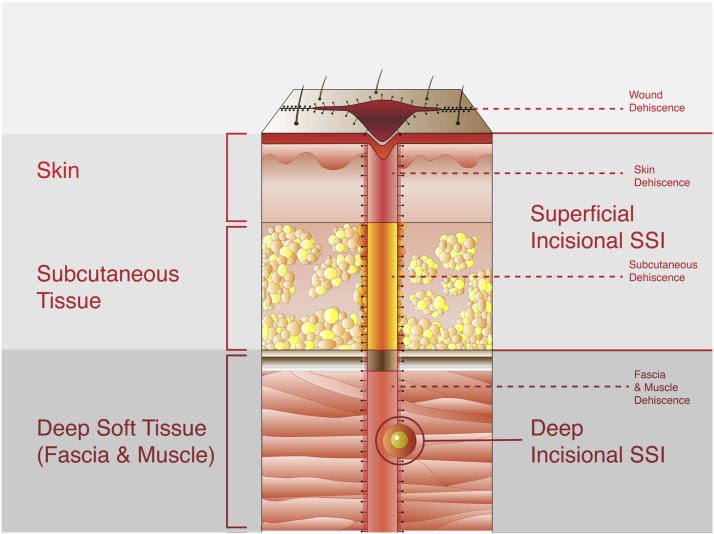
Conclusions: Wound complications such as SSI and dehiscence remain a significant source of morbidity following spine tumor surgery. Triaging patients on an individualized basis according to risk factors for complication may aid in selecting appropriate prophylactic strategies to prevent these complications. Future research in this area is still needed to strengthen recommendations.
Keywords: clinical algorithm; spinal oncology; spine surgery; surgical site infection; wound dehiscence.
Conflict of interest statement
Declaration of Conflicting InterestsThe author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors disclose no financial conflicts of interest directly pertinent to this work. Please see supplemental ICMJE documents for full disclosures.
Figures
Similar articles
-
Vesicoureteral Reflux.2024 Apr 30. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Apr 30. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 33085409 Free Books & Documents.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Paraspinous Muscle Flaps for the Treatment of Complex Spinal Wounds.Spine (Phila Pa 1976). 2020 May 1;45(9):599-604. doi: 10.1097/BRS.0000000000003341. Spine (Phila Pa 1976). 2020. PMID: 31770321
-
Building consensus: development of a Best Practice Guideline (BPG) for surgical site infection (SSI) prevention in high-risk pediatric spine surgery.J Pediatr Orthop. 2013 Jul-Aug;33(5):471-8. doi: 10.1097/BPO.0b013e3182840de2. J Pediatr Orthop. 2013. PMID: 23752142
-
Selection pressures of vancomycin powder use in spine surgery: a meta-analysis.Spine J. 2019 Jun;19(6):1076-1084. doi: 10.1016/j.spinee.2019.01.002. Epub 2019 Jan 17. Spine J. 2019. PMID: 30660741
Cited by
-
Evaluation of Adverse Events and the Impact on Health-Related Outcomes in Patients Undergoing Surgery for Metastatic Spine Tumors: Analysis of the Metastatic Tumor Research and Outcomes Network (MTRON) Registry Dataset.Global Spine J. 2025 Jun 6:21925682251347247. doi: 10.1177/21925682251347247. Online ahead of print. Global Spine J. 2025. PMID: 40480956 Free PMC article.
