

Coronary Artery Calcium Scores After Prophylactic Premenopausal Bilateral Salpingo-Oophorectomy
- PMID: 39801648
- PMCID: PMC11711998
- DOI: 10.1016/j.jaccao.2024.09.011
Coronary Artery Calcium Scores After Prophylactic Premenopausal Bilateral Salpingo-Oophorectomy
Abstract
Background: Premenopausal risk-reducing salpingo-oophorectomy (RRSO) in women at high familial risk of ovarian cancer leads to immediate menopause. Although early natural menopause is associated with increased cardiovascular disease risk, evidence on long-term cardiovascular disease risk after early surgical menopause is scarce.
Objectives: We sought to determine the long-term influence of the timing of RRSO on the development of coronary artery calcium (CAC), an established marker for cardiovascular disease risk.
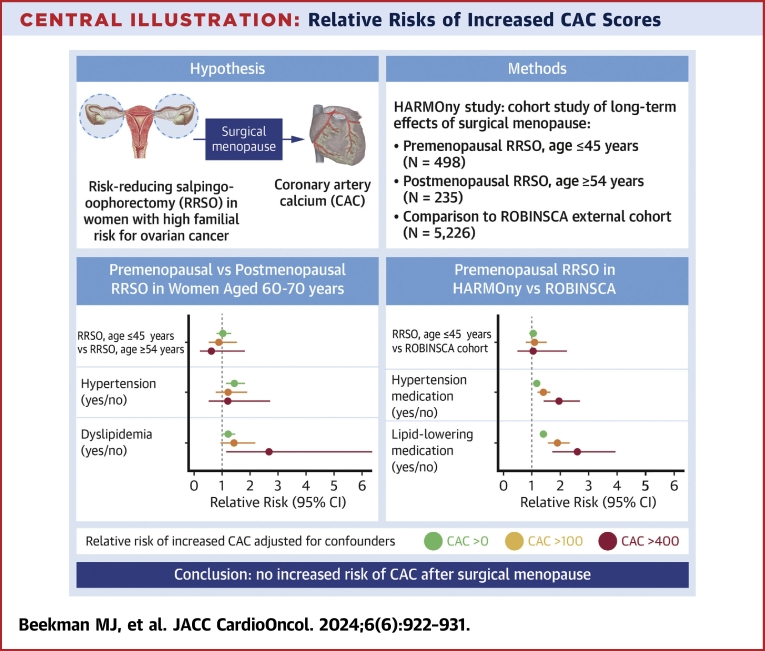
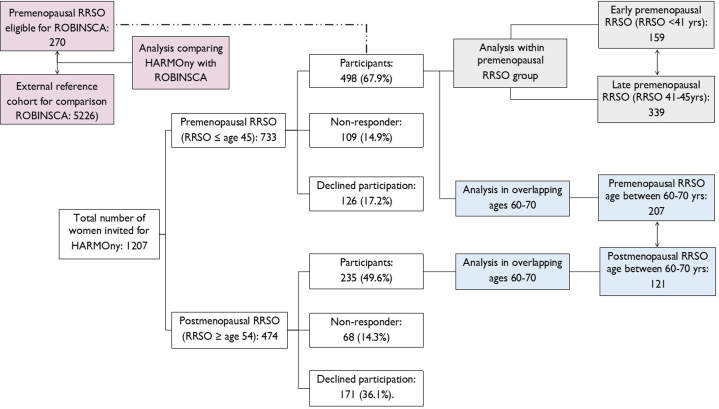
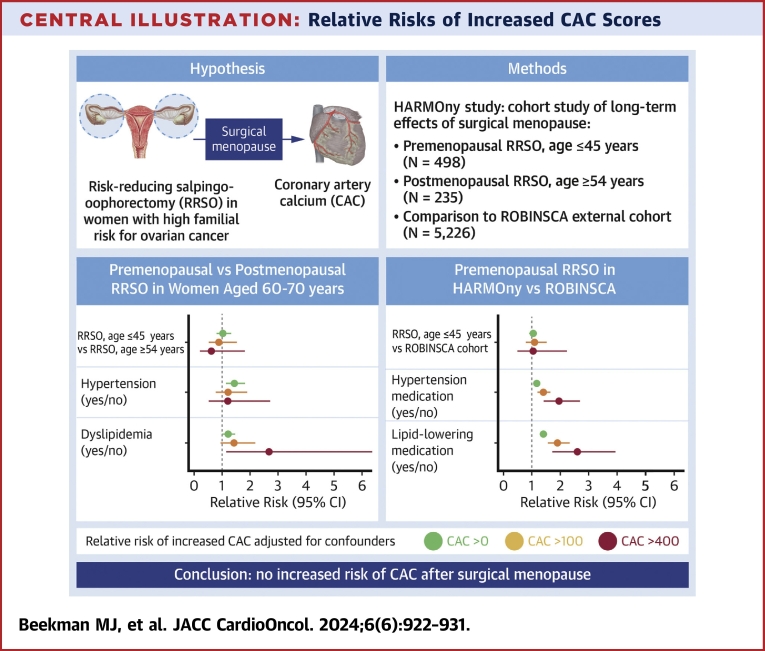
Methods: We conducted a cross-sectional study (N = 733) nested in a nationwide cohort of women at high familial risk of ovarian cancer. In women aged 60-70 years (n = 328), we compared CAC scores between women with a premenopausal RRSO (age ≤45 years) and women with a postmenopausal RRSO (age ≥54 years), using multivariable Poisson analyses. Within the premenopausal RRSO group (n = 498), we also examined the effect of age at RRSO. In addition, we compared the premenopausal RRSO group with an external reference cohort (n = 5,226).
Results: Multivariable analyses showed that the prevalence rates of any CAC (CAC >0), at least moderate CAC (CAC >100), and severe CAC (CAC >400) were comparable between the premenopausal and postmenopausal RRSO groups (relative risk [RR]: 0.93; 95% CI: 0.75-1.15 for any CAC; RR: 0.71; 95% CI: 0.43-1.17 for at least moderate CAC; RR: 0.81; 95% CI: 0.30-2.13 for severe CAC). There was no difference in CAC between the premenopausal RRSO group and a similar aged reference cohort. Timing of premenopausal RRSO (early premenopausal RRSO [<41 years] vs late premenopausal RRSO [41-45 years]) did not affect the outcomes.
Conclusions: Our results do not show a long-term adverse effect of surgical menopause on the development of CAC.
Keywords: BRCA; CAC; RRSO; cardiovascular disease; ovarian cancer; surgical menopause.
© 2024 The Authors.
Conflict of interest statement
The Dutch Cancer Society (KWF) and the Maarten van der Weijden foundation funded this project, registered under grant 10164. The funding body had no role in the design of the study, collection, analysis or interpretation of data or in writing the paper. Dr van der Aalst has received an advanced research grant for ROBINSCA by the European Research Council. Dr Budde has received institutional support to the radiology department of the Erasmus Medical Center by Siemens and HeartFlow; payments to the Erasmus MC for lectures by Bayer and Siemens; and serves unpaid as board member of the European Society of Cardiovascular Radiology and the editorial boards of Radiology: Cardiothoracic Imaging, EHJ Digital Health, and Journal of Hybrid Imaging. Dr de Jong has received research support to the department of radiology of UMC Utrecht by Philips Healthcare. Dr Vliegenthart has received institutional research grants by Siemens Healthineers, Dutch Heart Foundation, Dutch Cancer Foundation, and Netherlands organization for Health Research and Development; speaker fees by Siemens Healthineers and Bayer Healthcare; participates in the strategic advisory board of the Institute for Cardiometabolism and Nutrition; and is president of the European Society of Cardiovascular Radiology. Dr Ausems has received institutional payments by AstraZeneca. Dr de Koning has received institutional grants for the 4-in-the-lung-run trial HORIZON 2020. Dr Maas has received speaker fees by Novartis, Organon and Omron. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Henderson J.T., Webber E.M., Sawaya G.F. Screening for ovarian cancer: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2018;319(6):595–606. - PubMed
-
- Daly M.B., Pal T., Berry M.P., et al. Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2021;19(1):77–102. - PubMed
LinkOut - more resources
Full Text Sources
