

Mesenchymal stem cells for osteoarthritis: Recent advances in related cell therapy
- PMID: 39801757
- PMCID: PMC11711223
- DOI: 10.1002/btm2.10701
Mesenchymal stem cells for osteoarthritis: Recent advances in related cell therapy
Abstract
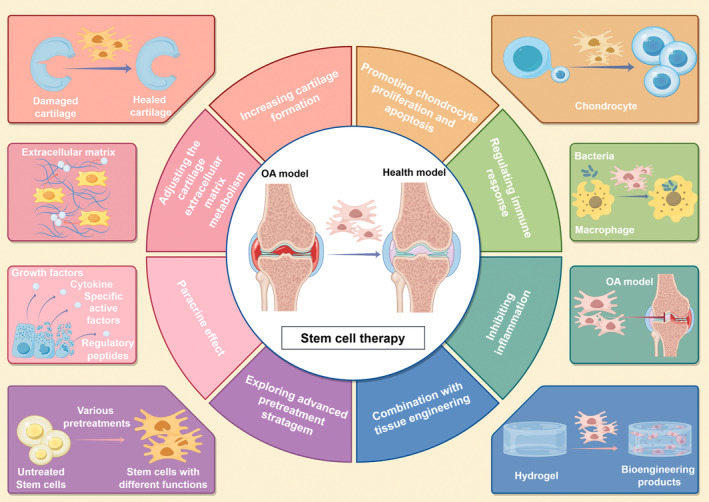
Osteoarthritis (OA) is a degenerative joint disease that affects the entire joint and has been a huge burden on the health care system worldwide. Although traditional therapy and targeted cartilage cell therapy have made significant progress in the treatment of OA and cartilage regeneration, there are still many problems. Mesenchymal stem cells from various tissues are the most studied cell type and have been used in preclinical and clinical studies of OA, because they are more widely available, have a greater capacity for in vitro expansion, and have anti-inflammatory and immunomodulatory properties compared to autologous chondrocytes. This article will systematically review the latest developments in these areas. It may provide new insights for improving OA and cartilage regeneration.
Keywords: cartilage; extracellular vesicles; mesenchymal stem cells; osteoarthritis; stem cell.
© 2024 The Author(s). Bioengineering & Translational Medicine published by Wiley Periodicals LLC on behalf of American Institute of Chemical Engineers.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


Similar articles
-
The Role of Extracellular Vesicles in the Pathogenesis, Diagnosis, and Treatment of Osteoarthritis.Molecules. 2021 Aug 17;26(16):4987. doi: 10.3390/molecules26164987. Molecules. 2021. PMID: 34443573 Free PMC article. Review.
-
Harnessing knee joint resident mesenchymal stem cells in cartilage tissue engineering.Acta Biomater. 2023 Sep 15;168:372-387. doi: 10.1016/j.actbio.2023.07.024. Epub 2023 Jul 21. Acta Biomater. 2023. PMID: 37481194 Review.
-
Chondrocyte and mesenchymal stem cell-based therapies for cartilage repair in osteoarthritis and related orthopaedic conditions.Maturitas. 2014 Jul;78(3):188-98. doi: 10.1016/j.maturitas.2014.04.017. Epub 2014 May 2. Maturitas. 2014. PMID: 24855933 Review.
-
The Role of Cartilage Stem/Progenitor Cells in Cartilage Repair in Osteoarthritis.Curr Stem Cell Res Ther. 2023;18(7):892-903. doi: 10.2174/1574888X17666221006113739. Curr Stem Cell Res Ther. 2023. PMID: 36201278 Free PMC article.
-
Cartilage Repair by Mesenchymal Stem Cell-Derived Exosomes: Preclinical and Clinical Trial Update and Perspectives.Adv Exp Med Biol. 2021;1326:73-93. doi: 10.1007/5584_2021_625. Adv Exp Med Biol. 2021. PMID: 33629260
Cited by
-
Construction of organoids using bioprinting technology: a frontier exploration of cartilage repair.J Orthop Translat. 2025 Jul 16;54:37-50. doi: 10.1016/j.jot.2025.06.020. eCollection 2025 Sep. J Orthop Translat. 2025. PMID: 40703568 Free PMC article. Review.
-
Future perspectives: advances in bone/cartilage organoid technology and clinical potential.Biomater Transl. 2024 Nov 15;5(4):425-443. doi: 10.12336/biomatertransl.2024.04.007. eCollection 2024. Biomater Transl. 2024. PMID: 39872930 Free PMC article. Review.
-
The Use of MSCs, iPSCs, and EVs in the Repair of Human MSK Tissues: Is Ultimate Success Dependent on Developing Excellent Implant Materials as Well as Creating an Optimal Environment for Implantation? What Is the Rationale for These Choices?Int J Mol Sci. 2025 Jun 28;26(13):6250. doi: 10.3390/ijms26136250. Int J Mol Sci. 2025. PMID: 40650028 Free PMC article. Review.
-
Autologous Versus Allogeneic Adipose-Derived Mesenchymal Stem Cell Therapy for Knee Osteoarthritis: A Systematic Review, Pairwise and Network Meta-Analysis of Randomized Controlled Trials.Cureus. 2025 Apr 21;17(4):e82713. doi: 10.7759/cureus.82713. eCollection 2025 Apr. Cureus. 2025. PMID: 40400817 Free PMC article. Review.
-
Unraveling Osteoarthritis: Mechanistic Insights and Emerging Therapies Targeting Pain and Inflammation.Biomolecules. 2025 Jun 16;15(6):874. doi: 10.3390/biom15060874. Biomolecules. 2025. PMID: 40563514 Free PMC article. Review.
References
-
- Hunter DJ, March L, Chew M. Osteoarthritis in 2020 and beyond: a lancet commission. Lancet. 2020;396(10264):1711‐1712. - PubMed
-
- Hunter DJ, Schofield D, Callander E. The individual and socioeconomic impact of osteoarthritis. Nat Rev Rheumatol. 2014;10(7):437‐441. - PubMed
-
- Hunter DJ, Bierma‐Zeinstra S. Osteoarthritis. Lancet. 2019;393(10182):1745‐1759. - PubMed
-
- Tang X, Wang S, Zhan S, et al. The prevalence of symptomatic knee osteoarthritis in China: results from the China health and retirement longitudinal study. Arthritis Rheumatol. 2016;68(3):648‐653. - PubMed
-
- Sharma L. Osteoarthritis of the knee. N Engl J Med. 2021;384(1):51‐59. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
