

Identifying biomarker-driven subphenotypes of cardiogenic shock: analysis of prospective cohorts and randomized controlled trials
- PMID: 39802301
- PMCID: PMC11718329
- DOI: 10.1016/j.eclinm.2024.103013
Identifying biomarker-driven subphenotypes of cardiogenic shock: analysis of prospective cohorts and randomized controlled trials
Abstract
Background: Cardiogenic shock (CS) is a heterogeneous clinical syndrome, making it challenging to predict patient trajectory and response to treatment. This study aims to identify biological/molecular CS subphenotypes, evaluate their association with outcome, and explore their impact on heterogeneity of treatment effect (ShockCO-OP, NCT06376318).
Methods: We used unsupervised clustering to integrate plasma biomarker data from two prospective cohorts of CS patients: CardShock (N = 205 [2010-2012, NCT01374867]) and the French and European Outcome reGistry in Intensive Care Units (FROG-ICU) (N = 228 [2011-2013, NCT01367093]) to determine the optimal number of classes. Thereafter, a simplified classifier (Euclidean distances) was used to assign the identified CS subphenotypes in three completed randomized controlled trials (RCTs) (OptimaCC, N = 57 [2011-2016, NCT01367743]; DOREMI, N = 192 [2017-2020, NCT03207165]; and CULPRIT-SHOCK, N = 434 [2013-2017, NCT01927549]) and explore heterogeneity of treatment effect with respect to 28-day mortality (primary outcome).
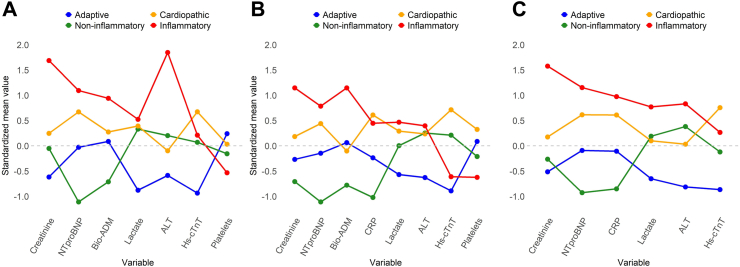
Findings: Four biomarker-driven CS subphenotypes ('adaptive', 'non-inflammatory', 'cardiopathic', and 'inflammatory') were identified separately in the two cohorts. Patients in the inflammatory and cardiopathic subphenotypes had the highest 28-day mortality (p (log-rank test) = 0.0099 and 0.0055 in the CardShock and FROG-ICU cohorts, respectively). Subphenotype membership significantly improved risk stratification when added to traditional risk factors including the Society for Cardiovascular Angiography and Interventions (SCAI) shock stages (increase in Harrell's C-index by 4% (p = 0.033) and 6% (p = 0.0068) respectively in the CardShock and the FROG-ICU cohorts). The simplified classifier identified CS subphenotypes with similar biological/molecular and outcome characteristics in the three independent RCTs. No significant interaction was observed between treatment effect and subphenotypes.
Interpretation: Subphenotypes with the highest concentration of biomarkers of endothelial dysfunction and inflammation (inflammatory) or myocardial injury/fibrosis (cardiopathic) were associated with mortality independently from the SCAI shock stages.
Funding: Dr Sabri Soussi was awarded the Canadian Institutes of Health Research (CIHR) Doctoral Foreign Study Award (DFSA) and the Merit Awards Program (Department of Anesthesiology and Pain Medicine, University of Toronto, Canada) for the current study.
Keywords: Cardiogenic shock; Critical care; Heterogeneity of treatment effect; Precision medicine; Unsupervised learning.
© 2024 The Author(s).
Conflict of interest statement
None of the authors of this paper has a financial or personal relationship with other persons or organizations that could inappropriately influence or bias the content of the paper. Dr. C.J. received honoraria for lectures/presentations from Bristol Myers Squibb (New York, US), Edwards Lifesciences (Irvine, California, US), Daichi Sankyo (Tokyo, Japan) and Boehringer-Ingelheim (Ingelheim, Germany). He received grants or had contracts with the German research foundation, the German ministry for economy and energy, the State of Nordrhine-Westfalia, the German space agency, the European Union and Edwards Lifescience (Irvine, California, US). He had leadership or fiduciary role in the German cardiac society, the German society for internal medicine, the German society for medical intensive care and the European society for intensive care medicine. Dr. H.T. had leadership or fiduciary role in the German cardiac society. Dr. J.P. received travel support to attend meetings from Overcome GmbH (Paris, France). She received grants or had contracts with the German cardiac society, the German society for heart research, Dr. Rolf Schwiete Foundation and Maquet Cardiopulmonary (Baden-Württemberg, Germany). Dr. E.G. received fees as a member of the advisory boards and/or steering committees and/or from research grants from Magnisense (Paris, France), Adrenomed (Hennigsdorf, Germany) and Deltex Medical (Chichester, United Kingdom). Dr. A.M. has received speaker's honoraria from Merck (Darmstadt, Germany), Medtronik (Dublin, Ireland), Viatris (Canonsburg, US), Novartis (Basel, Switzerland), Roche (Basel, Switzerland), Bayer (Leverkusen, Germany) and Astra Zeneca (Cambridge, UK); and fees as a member of the advisory boards and/or steering committees and/or research grants from Adrenomed (Hennigsdorf, Germany), Corteria (Boca Raton, Florida, US), Roche (Basel, Switzerland), Fire1 (Dublin, Ireland), Sphyngotec (Hennigsdorf, Germany), Abbott (Chicago, Illinois), Bayer (Leverkusen, Germany), Implicity (Paris, France), Windtree (Warrington, Pennsylvania, US), S-Form Pharma (Brussels, Belgium), Implicity (Paris, France), 4TEEN4 (Hennigsdorf, Germany) and the French government. He received equipment/material from Sphyngotec (Hennigsdorf, Germany). He is co-inventor of a patent (owned by S-Form pharma) on combination therapy for patients having acute or persistent dyspnea. The remaining authors declare no competing interests.
Figures




References
-
- Arrigo M., Price S., Baran D.A., et al. Optimising clinical trials in acute myocardial infarction complicated by cardiogenic shock: a statement from the 2020 critical care clinical trialists workshop. Lancet Respir Med. 2021;9(10):1192–1202. - PubMed
-
- Sarma D., Jentzer J.C., Soussi S. Cardiogenic shock: a major challenge for the clinical trialist. Curr Opin Crit Care. 2023;29(4):371–380. - PubMed
-
- Jentzer J.C., Ahmed A.M., Vallabhajosyula S., et al. Shock in the cardiac intensive care unit: changes in epidemiology and prognosis over time. Am Heart J. 2021;232:94–104. - PubMed
-
- Lawler P.R., Mehra M.R. Advancing from a “hemodynamic model” to a “mechanistic disease-modifying model” of cardiogenic shock. J Heart Lung Transplant. 2018;37(11):1285–1288. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
