

This is a preprint.
Demographics, Epidemiology, Mortality, and Difficult-To-Treat Resistance Patterns of Bacterial Bloodstream Infections in the Global United States Military Health System from 2010-2019: A Retrospective Cohort Study
- PMID: 39802776
- PMCID: PMC11722484
- DOI: 10.1101/2024.10.02.24314780
Demographics, Epidemiology, Mortality, and Difficult-To-Treat Resistance Patterns of Bacterial Bloodstream Infections in the Global United States Military Health System from 2010-2019: A Retrospective Cohort Study
Update in
-
Demographics, epidemiology, mortality and difficult-to-treat resistance patterns of bacterial bloodstream infections in the global US Military Health System from 2010 to 2019: a retrospective cohort study.BMJ Open. 2025 Mar 3;15(3):e094861. doi: 10.1136/bmjopen-2024-094861. BMJ Open. 2025. PMID: 40032367 Free PMC article.
Abstract
Objective: To describe demographics, causative pathogens, hospitalization, mortality, and antimicrobial resistance of bacterial bloodstream infections (BSIs) among beneficiaries in the global U.S. Military Health System (MHS), a single-provider healthcare system with 10-year longitudinal follow-up.
Design: Retrospective cohort study.
Setting: Clinical and demographic data collected from the MHS Data Repository and collated with microbiological data obtained from the Defense Centers for Public Health-Portsmouth.
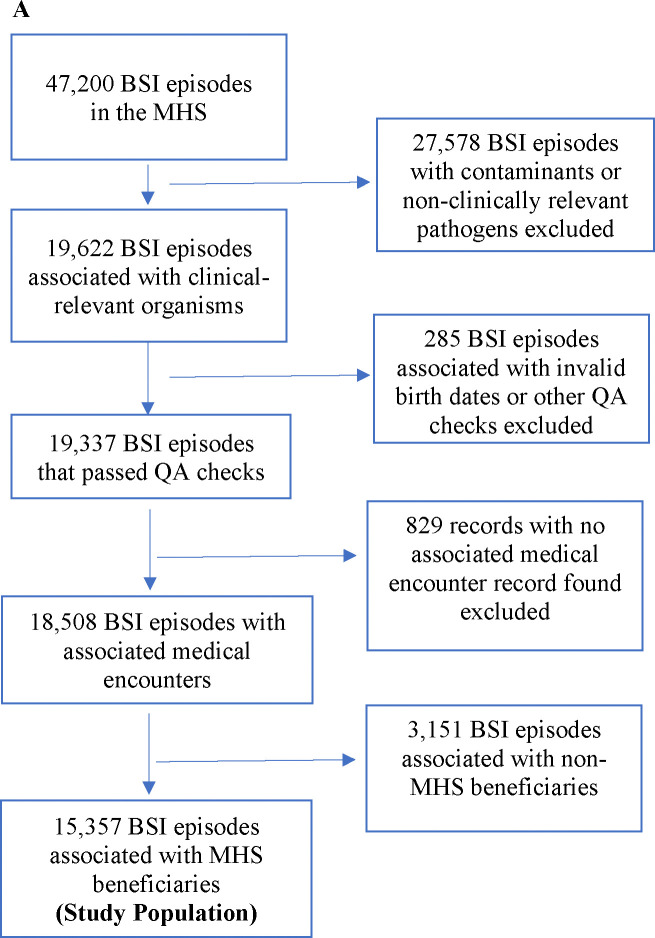
Participants: 12,748 MHS beneficiaries diagnosed with 15,357 bacterial BSIs (2010-2019).
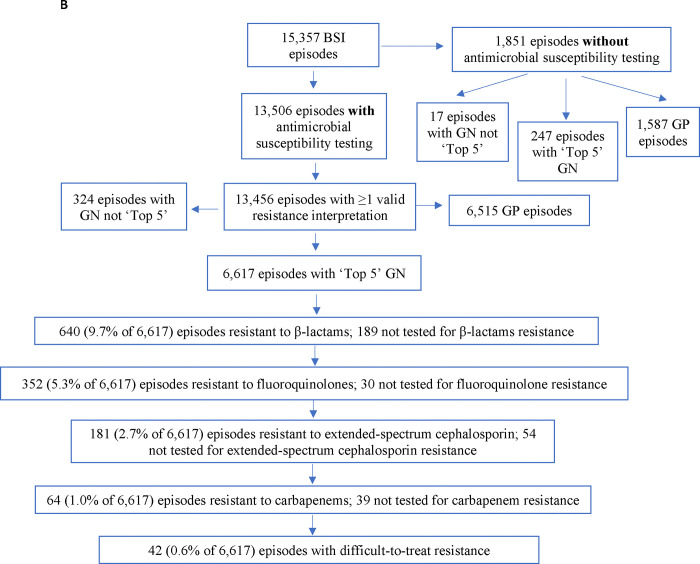
Main outcomes and measures: Demographic data and diagnosis codes preceding BSI episodes and during hospitalizations were collected. Inpatient admission data identified acute clinical diagnoses, intensive care unit (ICU) admission, and mortality. BSI pathogens were evaluated for antimicrobial resistance, including difficult-to-treat resistance (DTR). Crude mortality trends were assessed.
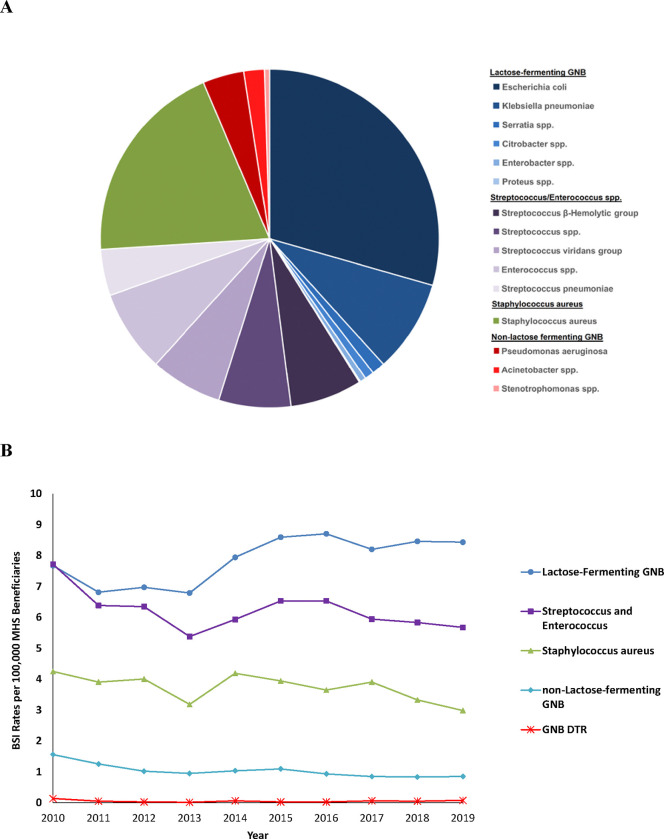
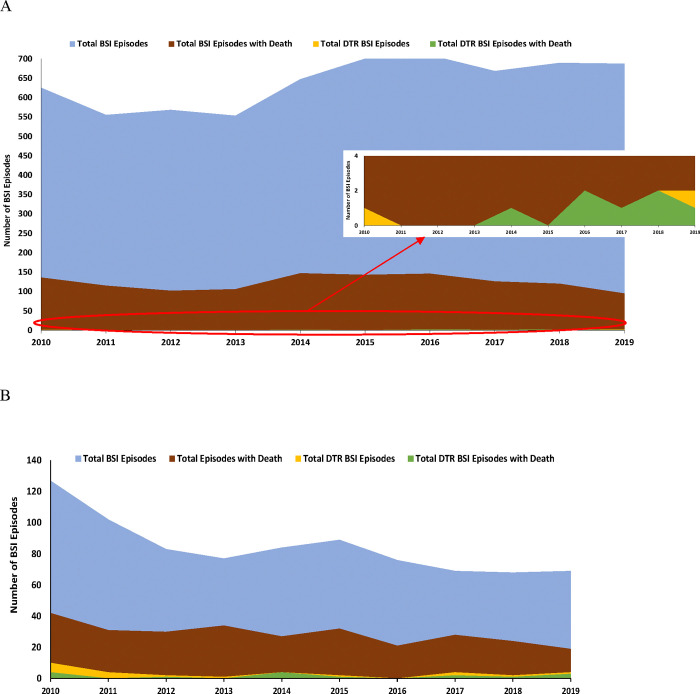
Results: The decade analyzed included 15,357 BSI episodes in 12,748 patients; 6,216 patients (48.8%) were ≥65 years and 83.7% of episodes had ≥1 comorbidity (12,856 of 15,357). Approximately 29% of episodes with hospitalization required ICU admission and ~34% had concurrent urinary tract infections. Pathogen distribution was 53% and 47% for Gram-positive bacteria and Gram-negative bacilli (GNB), respectively. Inpatient mortality was 4.4%, and at one year was 23.4%; 0.5% (16 of 2,977) of deaths were associated with DTR GNB. Among an average 8,145,778 individuals receiving care annually in the MHS, annual rates of overall BSI, methicillin-resistant Staphylococcus aureus, vancomycin-resistant Enterococcus spp., and DTR GNB BSI were 18.9, 1.30, 0.25, and 0.05 per 100,000 beneficiaries, respectively. Over the decade, annual mortality did not significantly increase for any pathogen and decreased by ~3% for lactose-fermenting GNB BSI (p=0.048).
Conclusions: In the global U.S. MHS, mortality burden associated with BSI was substantial (approximately 1 in 4 dying at 1 year), relatively unchanged over a decade, and associated with older age and comorbidities. First-line treatment options remained available for 99.7% of BSIs. Population-level improvements in BSI survival might be maximally influenced by focusing on prevention, early detection, prompt antibiotics, and other novel therapies not contingent on in vitro activity.
Conflict of interest statement
Competing Interests: All authors have completed the ICMJE uniform disclosure form at http://www.icmje.org/disclosure-of-interest/ and declare: MG, CM, MLC, EP, and KM received grants through their institution for this study as reported in the funding statement. MLC also received funding from USU through her institution for a separate research protocol during the past 36 months. JHP received consulting fees from Adaptive Phage Therapeutics, Arrevus Inc., Atheln Inc., Eicos Sciences, Eyecheck Inc., GlaxoSmithKline plc, Ray Therapeutics Inc., Resolve, Romark, Spine BioPharma Inc., Shionogi Inc., Utility Therapeutics, and Vir Biotechnology Inc. JHP is an unpaid board member of Health Literacy Media. ACV and CL are active-duty service members and they and their dependents received healthcare via the MHS during the study period and were included in the study as patients. SSK, SW, UC, BP, NS, DF, and JW declare no completing interests.
Figures
References
-
- Torio CM, Moore BJ. National inpatient hospital costs: the most expensive conditions by payer, 2013: Statistical Brief #204. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Rockville, MD, 2006. - PubMed
-
- Wisplinghoff H, Bischoff T, Tallent SM, Seifert H, Wenzel RP, Edmond MB. Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study. Clin Infect Dis 2004;39:309–17. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous