

This is a preprint.
Immune Checkpoint Molecules as Biomarkers of Staphylococcus aureus Bone Infection and Clinical Outcome
- PMID: 39803468
- PMCID: PMC11722373
- DOI: 10.1101/2024.12.30.630837
Immune Checkpoint Molecules as Biomarkers of Staphylococcus aureus Bone Infection and Clinical Outcome
Abstract
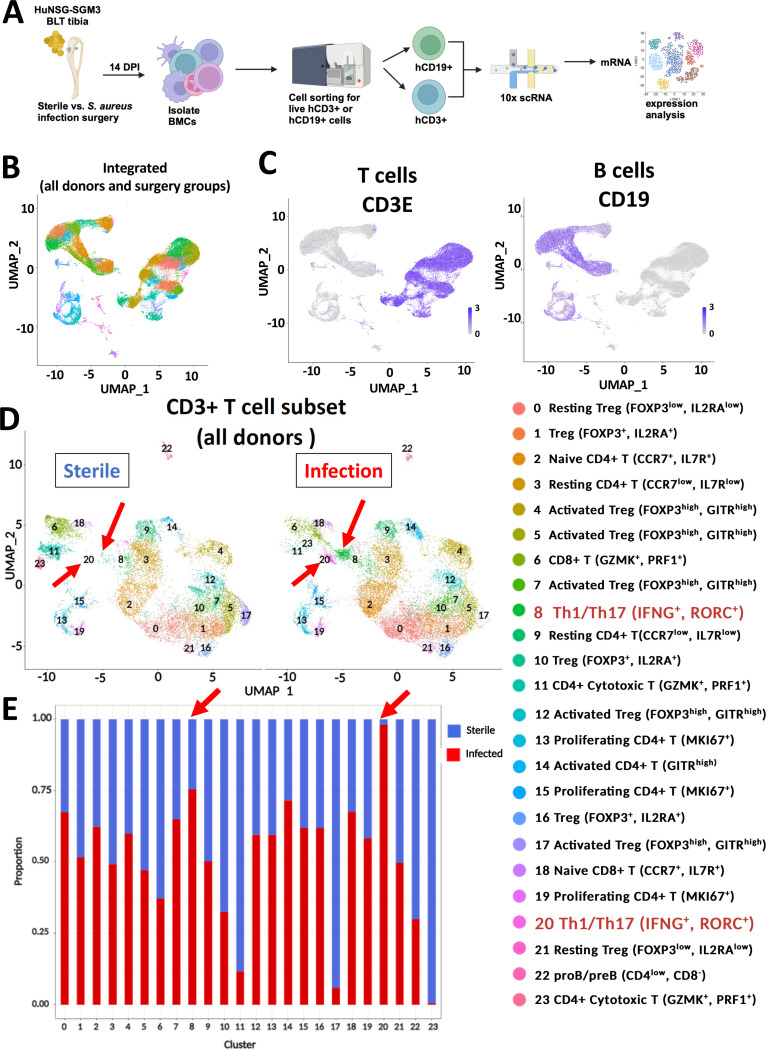
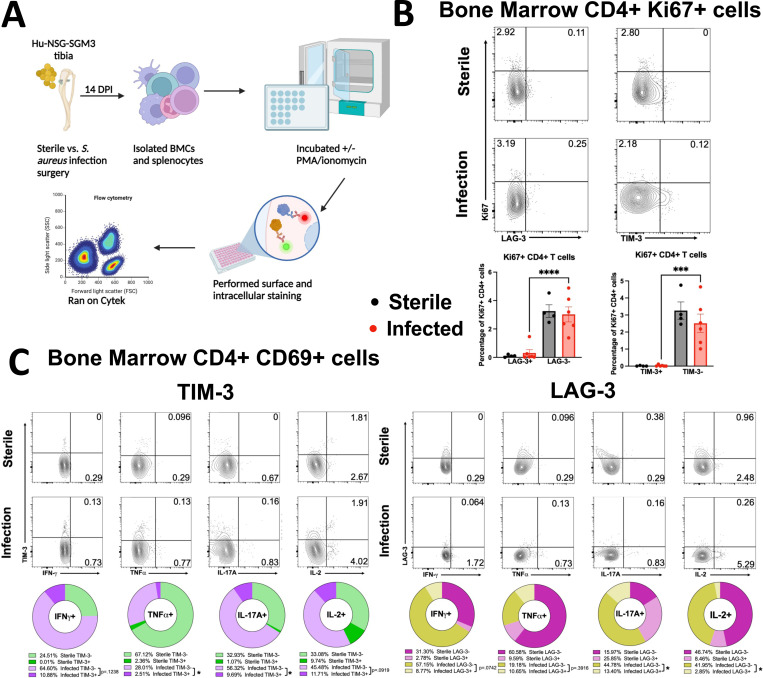
Staphylococcus aureus prosthetic joint infections (PJIs) are broadly considered incurable, and clinical diagnostics that guide conservative vs. aggressive surgical treatments don't exist. Multi-omics studies in a humanized NSG-SGM3 BLT mouse model demonstrate human T cells: 1) are remarkably heterogenous in gene expression and numbers, and 2) exist as a mixed population of activated, progenitor-exhausted, and terminally-exhausted Th1/Th17 cells with increased expression of immune checkpoint proteins (LAG3, TIM-3). Importantly, these proteins are upregulated in the serum and the bone marrow of S. aureus PJI patients. A multiparametric nomogram combining high serum immune checkpoint protein levels with low proinflammatory cytokine levels (IFN-γ, IL-2, TNF-α, IL-17) revealed that TIM-3 was highly predictive of adverse disease outcomes (AUC=0.89). Hence, T cell impairment in the form of immune checkpoint expression and exhaustion could be a functional biomarker for S. aureus PJI disease outcome, and blockade of checkpoint proteins could potentially improve outcomes following surgery.
Keywords: Staphylococcus aureus; T cell exhaustion; host-pathogen interactions; immune checkpoint proteins; osteomyelitis; scRNAseq.
Conflict of interest statement
Conflict of interest statement GM, EMS, and MS are inventors of a patent application filed by the University of Rochester and are currently under an exclusive licensing agreement with TEx Immunetics Inc. (TEX). GM and AG are co-founders of TEX and have stock in TEX. All other authors declare that no conflict of interest exists.
Figures





References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials