

Cognitive stimulation to improve cognitive functioning in people with dementia
- PMID: 39804128
- PMCID: PMC9891430
- DOI: 10.1002/14651858.CD005562.pub3
Cognitive stimulation to improve cognitive functioning in people with dementia
Abstract
Background: Cognitive stimulation (CS) is an intervention for people with dementia offering a range of enjoyable activities providing general stimulation for thinking, concentration and memory, usually in a social setting, such as a small group. CS is distinguished from other approaches such as cognitive training and cognitive rehabilitation by its broad focus and social elements, aiming to improve domains such as quality of life (QoL) and mood as well as cognitive function. Recommended in various guidelines and widely implemented internationally, questions remain regarding different modes of delivery and the clinical significance of any benefits. A systematic review of CS is important to clarify its effectiveness and place practice recommendations on a sound evidence base. This review was last updated in 2012.
Objectives: To evaluate the evidence for the effectiveness of CS for people with dementia, including any negative effects, on cognition and other relevant outcomes, accounting where possible for differences in its implementation.
Search methods: We identified trials from a search of the Cochrane Dementia and Cognitive Improvement Group Specialized Register, last searched on 3 March 2022. We used the search terms: cognitive stimulation, reality orientation, memory therapy, memory groups, memory support, memory stimulation, global stimulation, cognitive psychostimulation. We performed supplementary searches in a number of major healthcare databases and trial registers to ensure the search was up-to-date and comprehensive.
Selection criteria: We included all randomised controlled trials (RCTs) of CS for dementia published in peer review journals in the English language incorporating a measure of cognitive change.
Data collection and analysis: We used standard methodological procedures expected by Cochrane. As CS is a psychosocial intervention, we did not expect those receiving or delivering CS to be blinded to the nature of the intervention. Where necessary, we contacted study authors requesting data not provided in the papers. Where appropriate, we undertook subgroup analysis by modality (individual versus group), number of sessions and frequency, setting (community versus care home), type of control condition and dementia severity. We used GRADE methods to assess the overall quality of evidence for each outcome.
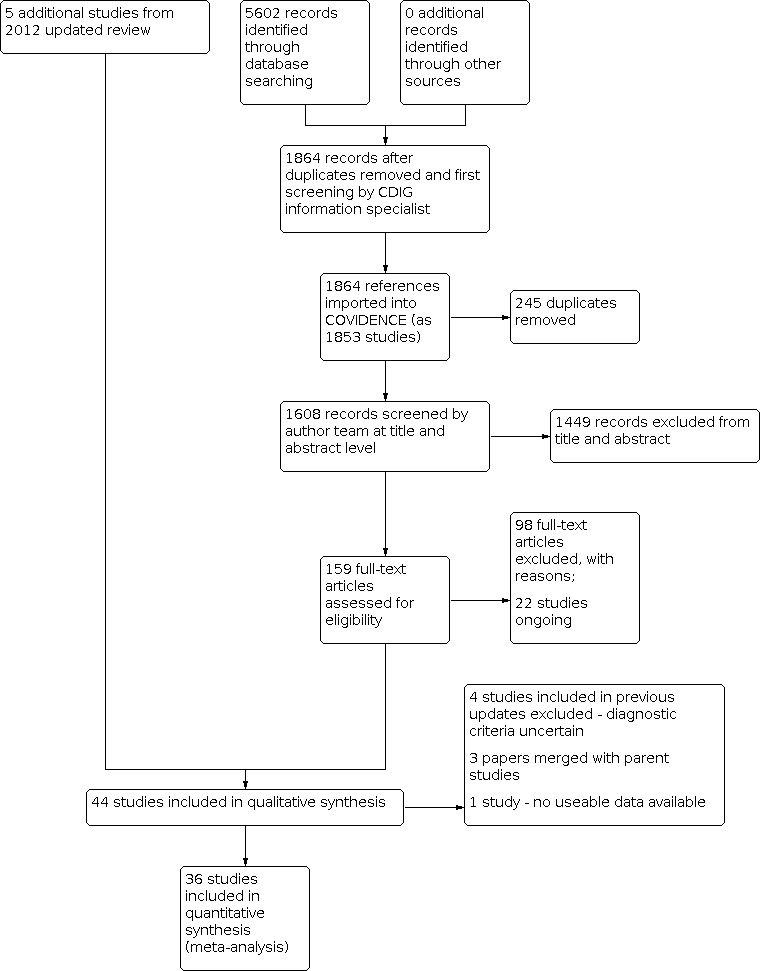
Main results: We included 37 RCTs (with 2766 participants), 26 published since the previous update. Most evaluated CS groups; eight examined individual CS. Participants' median age was 79.7 years. Sixteen studies included participants resident in care homes or hospitals. Study quality showed indications of improvement since the previous review, with few areas of high risk of bias. Assessors were clearly blinded to treatment allocation in most studies (81%) and most studies (81%) reported use of a treatment manual by those delivering the intervention. However, in a substantial number of studies (59%), we could not find details on all aspects of the randomisation procedures, leading us to rate the risk of selection bias as unclear. We entered data in the meta-analyses from 36 studies (2704 participants; CS: 1432, controls: 1272). The primary analysis was on changes evident immediately following the treatment period (median length 10 weeks; range 4 to 52 weeks). Only eight studies provided data allowing evaluation of whether effects were subsequently maintained (four at 6- to 12-week follow-up; four at 8- to 12-month follow-up). No negative effects were reported. Overall, we found moderate-quality evidence for a small benefit in cognition associated with CS (standardised mean difference (SMD) 0.40, 95% CI 0.25 to 0.55). In the 25 studies, with 1893 participants, reporting the widely used MMSE (Mini-Mental State Examination) test for cognitive function in dementia, there was moderate-quality evidence of a clinically important difference of 1.99 points between CS and controls (95% CI: 1.24, 2.74). In secondary analyses, with smaller total sample sizes, again examining the difference between CS and controls on changes immediately following the intervention period, we found moderate-quality evidence of a slight improvement in self-reported QoL (18 studies, 1584 participants; SMD: 0.25 [95% CI: 0.07, 0.42]) as well as in QoL ratings made by proxies (staff or caregivers). We found high-quality evidence for clinically relevant improvements in staff/interviewer ratings of communication and social interaction (5 studies, 702 participants; SMD: 0.53 [95% CI: 0.36, 0.70]) and for slight benefits in instrumental Activities of Daily Living, self-reported depressed mood, staff/interviewer-rated anxiety and general behaviour rating scales. We found moderate-quality evidence for slight improvements in behaviour that challenges and in basic Activities of Daily Living and low-quality evidence for a slight improvement in staff/interviewer-rated depressed mood. A few studies reported a range of outcomes for family caregivers. We found moderate-quality evidence that overall CS made little or no difference to caregivers' mood or anxiety. We found a high level of inconsistency between studies in relation to both cognitive outcomes and QoL. In exploratory subgroup analyses, we did not identify an effect of modality (group versus individual) or, for group studies, of setting (community versus care home), total number of group sessions or type of control condition (treatment-as-usual versus active controls). However, we did find improvements in cognition were larger where group sessions were more frequent (twice weekly or more versus once weekly) and where average severity of dementia among participants at the start of the intervention was 'mild' rather than 'moderate'. Imbalance in numbers of studies and participants between subgroups and residual inconsistency requires these exploratory findings to be interpreted cautiously.
Authors' conclusions: In this updated review, now with a much more extensive evidence base, we have again identified small, short-term cognitive benefits for people with mild to moderate dementia participating in CS programmes. From a smaller number of studies, we have also found clinically relevant improvements in communication and social interaction and slight benefits in a range of outcomes including QoL, mood and behaviour that challenges. There are relatively few studies of individual CS, and further research is needed to delineate the effectiveness of different delivery methods (including digital and remote, individual and group) and of multi-component programmes. We have identified that the frequency of group sessions and level of dementia severity may influence the outcomes of CS, and these aspects should be studied further. There remains an evidence gap in relation to the potential benefits of longer-term CS programmes and their clinical significance.
배경: 인지 자극(CS)은 치매 환자를 위한 중재이다. 일반적으로 소그룹과 같은 사회적 환경에서 생각, 집중 및 기억에 대한 일반적인 자극을 줄 수 있도록 다양하고 즐거운 활동을 제공한다. CS(인지 자극)는 광범위한 초점과 사회적 요소에 의해 인지 훈련 및 인지 재활 같은 다른 접근법과 구별된다. 인지기능은 물론이고 삶의 질(QoL), 기분 같은 영역을 개선하는 것을 목표로 하고 있다. 다양한 지침에서 권장되고 국제적으로 널리 시행되고 있지만 다양한 전달 방식과 이점의 임상적 중요성에 대한 질문이 남아 있습니다. CS에 대한 체계적인 검토는 그 효과를 명확히 하고 건전한 근거 기반에 실제 권장 사항을 배치하는 데 중요합니다. 이 리뷰는 2012년에 마지막으로 업데이트되었습니다. 목적: 인지 및 기타 관련 결과에 대한 부정적인 영향을 포함하여 치매 환자에 대한 CS의 효과에 대한 증거를 평가하고 구현의 차이가 나는 지점을 파악하기 위함 검색 전략: 2022년 3월 3일에 마지막으로 검색된 Cochrane Dementia and Cognitive Improvement Group Specialized Register의 검색에서 임상시험을 식별했다. 우리는 인지 자극, 현실 지향, 기억 요법, 기억 그룹, 기억 지원, 기억 자극, 글로벌 자극, 인지 심리 자극과 같은 검색어를 사용했다. 검색이 최신이고 포괄적인지 확인하기 위해 여러 주요 의료 데이터베이스 및 시험 등록에서 보충 검색을 수행했다. 선정 기준: 인지 변화의 척도를 통합한 영문 피어 리뷰 저널에 발표된 치매에 대한 CS의 모든 무작위 대조 시험(RCT)을 포함했다. 자료 수집 및 분석: Cochrane에서 기대하는 표준 방법론적 절차를 사용했다. CS는 심리사회적 개입이기 때문에 CS를 받거나 전달하는 사람들이 중재의 본질에 대해 무지할 것이라고 기대하지 않았다. 필요한 경우 연구 저자에게 연락하여 논문에 제공되지 않은 데이터를 요청했다. 적절한 경우 적용(개인 대 그룹), 세션 수 및 빈도, 설정(커뮤니티 대 요양원), 제어 조건 유형 및 치매 중증도별로 하위 그룹 분석을 수행했다. 각 결과에 대한 전반적인 근거의 질을 평가하기 위해 GRADE(Grading of Recommendations, Assessment, Development, and Evaluation) 방법론을 사용했다. 주요 결과: 37개의 RCT(참가자 2766명)를 포함했으며, 이전 업데이트 이후 26편이 출판되었다. 대부분은 CS그룹으로 평가되었고 8명은 개인별 CS로 측정되었다. 참가자의 평균 나이는 79.7세였다. 16건의 연구에는 요양원이나 병원에 있는 참가자가 포함되었다. 비뚤림 위험이 높은 영역이 거의 없는 것을 보니 연구 품질은 이전 문헌고찰 이후 개선의 징후를 보여주었다. 평가자는 대부분의 연구(81%)에서 치료 할당에 대해 명확하게 눈가림을 했고 대부분의 연구(81%)는 중재를 제공하는 사람들이 치료 매뉴얼을 사용한다고 보고했다. 그러나 상당한 수의 연구(59%)에서 무작위화 절차의 모든 측면에 대한 세부 정보를 찾을 수 없었기 때문에 선택 비뚤림의 위험을 불분명한 것으로 평가했다. 우리는 36개의 연구로부터 얻은 데이터를 메타분석에 사용했다.(참가자 2,704명, CS중재: 1423명, 대조군: 1272명), 1차 분석은 치료 기간(중앙값 10주, 범위 4~52주) 직후 명백한 변화에 대한 것이었다. 8건의 연구만이 효과가 계속 유지되는지 여부를 평가할 수 있는 데이터를 제공했다(6~12주 추적 조사에서 4건, 8~12개월 추적 조사에서 4건). 부작용은 보고되지 않았다. 전반적으로 CS와 관련된 인지의 작은 이점에 대해 중간 정수준의 근거를 발견했다(표준화 평균 차이(SMD) 0.40, 95% CI(신뢰구간) 0.25~0.55). 1,893명의 참가자가 참여한 25건의 연구에서 치매의 인지 기능에 널리 사용되는 MMSE(Mini‐Mental State Examination) 테스트를 보고했으며, 근거의 확실성은 중간 정도로서. CS중재군과 대조군의 임상적으로 중요한 차이는 1.99점이었다(95% 신뢰구간: 1.24~2,74). 총 표본 크기가 더 작은 2차 분석에서 중재 기간 직후의 변화에 대한 CS중재군과 대조군의 차이를 다시 조사한 결과, 근거의 확실성이 중간정도로서 자가 보고 QoL(삶의 질)이 약간 개선된 것을 발견했다(18개 연구, 1584명 참여자, SMD: 0.25[95% 신뢰구간 0.07~0.42]). 대리인(직원 또는 간병인)이 만든 QoL 등급에서도 마찬가지였다. 의사소통 및 사회적 상호 작용에 대한 직원/면접관 평가에서 임상적으로 관련된 개선에 대해 근거의 확실성이 높았다(연구 5건, 참가자 702명; SMD: 0.53[95% 신뢰구간 0.36~ 0.70]). 도구적 일상 생활 활동, 자가 보고 우울 기분, 직원/면접관이 평가한 불안 및 일반 행동 평가 척도에서 약간의 이점이 있었다. 도전적인 행동과 일상 생활의 기본 활동에서 약간의 개선에 대한 근거의 확실성은 중간 정도였고 직원/면접관이 평가한 우울한 기분의 약간의 개선에 대한 근거의 확실성은 낮았다. 몇몇 연구에서는 가족 간병인에 대한 다양한 결과를 보고했다. 결국 CS가 간병인의 기분이나 불안에 거의 또는 전혀 차이가 없다는 근거의 확실성은 중간 정도였다. 인지 결과와 QoL 모두와 관련하여 연구 간에 높은 수준의 불일치가 있음을 발견했다. 탐색적 하위 그룹 분석에서 적용(그룹 대 개인) 또는 그룹 연구의 경우 설정(지역사회 대 요양원), 총 그룹 세션 수 또는 제어 조건 유형(평상시 치료 대 활발한 대조군)의 효과를 찾지 못하였다. 그러나 우리는 그룹 세션이 더 빈번한 경우(주 1회에 비해 주 2회 이상)와 중재 시작 시 참가자의 평균 치매 중증도가 '보통'이 아니라 '경증'인 경우에 인지 개선이 더 컸음을 발견했다. 하위 그룹 간의 연구 및 참여자 수의 불균형과 잔류자 수 불일치가 있었으니 이러한 탐색적 결과를 신중하게 해석해야 한다. 연구진 결론: 이제 훨씬 더 광범위한 증거 기반을 갖춘 이 업데이트된 고찰에서 우리는 CS 프로그램에 참여하는 경증에서 중등도 치매 환자를 위한 작은 단기 인지 혜택을 다시 확인했다. 더 적은 수의 연구에서 우리는 또한 의사소통 및 사회적 상호작용에서 임상적으로 관련된 개선을 발견했고 삶의 질, 도전적인 기분 및 행동을 포함한 다양한 결과에서 약간의 이점을 발견했다. 개별 CS에 대한 연구는 상대적으로 적고 다양한 전달 방법(디지털과 원격, 개인과 그룹 포함) 및 다중 구성 요소 프로그램의 효과를 설명하기 위해서는 추가 연구가 필요하다. 우리는 그룹 세션의 빈도와 치매 중증도가 CS의 결과에 영향을 미칠 수 있음을 확인했으며 이러한 측면은 추가 연구가 필요하다. 장기 CS 프로그램의 잠재적 이점과 임상적 중요성에 관련해서는 근거의 격차가 남아 있다.
บทนำ: การกระตุ้นความรู้ความเข้าใจ (CS) คือวิธีการที่ใช้ (intervention) สำหรับผู้ที่มีภาวะสมองเสื่อม โดยนำเสนอกิจกรรมที่สนุกสนานต่างๆ ซึ่งโดยทั่วไปช่วยกระตุ้นการคิด สมาธิ และความจำ ในสภาพแวดล้อมทางสังคม เช่น กลุ่มเล็กๆ CS แตกต่างจากแนวทางอื่นๆ เช่น การฝึกอบรมความรู้ความเข้าใจและการฟื้นฟูสมรรถภาพทางปัญญาโดยการเน้นการกระตุ้นกว้างๆและองค์ประกอบทางสังคม โดยมีเป้าหมายเพื่อปรับปรุงในบริบทต่างๆ เช่น คุณภาพชีวิต (QoL) และอารมณ์ ตลอดจนการทำงานของการรับรู้ มีการแนะนำในแนวทางต่าง ๆ และนำไปใช้อย่างกว้างขวางในระดับสากล แต่ยังมีคำถามเกี่ยวกับวิธีการดำเนินการที่แตกต่างกันและมีประโยชน์ที่มีความสำคัญทางคลินิกหรือไม่ การทบทวนอย่างเป็นระบบเป็นสิ่งสำคัญในการชี้แจงประสิทธิภาพและให้คำแนะนำการปฏิบัติไว้ตามหลักฐานที่น่าเชื่อถือ การทบทวนวรรณกรรมนี้ได้รับการปรับปรุงล่าสุดในปี 2012 วัตถุประสงค์: เพื่อประเมินหลักฐานสำหรับประสิทธิผลของ CS สำหรับผู้ที่มีภาวะสมองเสื่อม รวมถึงผลกระทบด้านลบใดๆ ต่อความรู้ความเข้าใจและผลลัพธ์อื่นๆ ที่เกี่ยวข้อง โดยคำนึงถึงความแตกต่างในการนำไปใช้หากเป็นไปได้ วิธีการสืบค้น: เราระบุการทดลองจากการค้นหา Cochrane Dementia and Cognitive Improvement Group Specialized Register ค้นหาล่าสุดเมื่อวันที่ 3 มีนาคม 2022 เราใช้คำค้นหา: การกระตุ้นความรู้ความเข้าใจ, การปฐมนิเทศความเป็นจริง, การบำบัดความจำ, กลุ่มความจำ, การสนับสนุนหน่วยความจำ, การกระตุ้นความจำ, การกระตุ้นโดยรวม, การกระตุ้นจิตทางปัญญา เราทำการค้นหาเพิ่มเติมในฐานข้อมูลด้านการดูแลสุขภาพที่สำคัญจำนวนหนึ่งและทะเบียนการทดลองเพื่อให้แน่ใจว่าการค้นหานั้นทันสมัยและครอบคลุม เกณฑ์การคัดเลือก: เรารวมการทดลองแบบสุ่มที่มีกลุ่มควบคุม (RCTs) ทั้งหมดของ CS สำหรับภาวะสมองเสื่อมที่ตีพิมพ์ในวารสารวิชาการเป็นภาษาอังกฤษ ซึ่งรวมการวัดการเปลี่ยนแปลงทางความคิด การรวบรวมและวิเคราะห์ข้อมูล: เราใช้ขั้นตอนวิธีการมาตรฐานที่ Cochrane กำหนด เนื่องจาก CS เป็นการแทรกแซงทางจิตสังคม เราไม่ได้คาดหวังว่าผู้ที่ได้รับหรือให้ CS จะถูกปกปิดกลุ่มของการแทรกแซง หากจำเป็น เราได้ติดต่อผู้เขียนการศึกษาเพื่อขอข้อมูลที่ไม่ได้ระบุไว้ในรายงาน ตามความเหมาะสม เราดำเนินการวิเคราะห์กลุ่มย่อยตามวิธีการ (รายบุคคลเทียบกับกลุ่ม) จำนวน sessions และความถี่ สถานที่ (ชุมชนและสถานดูแลเด็ก) ประเภทของเงื่อนไขการควบคุมและความรุนแรงของภาวะสมองเสื่อม และใช้วีธี GRADE เพื่อประเมินคุณภาพของงานวิจัยในแต่ละผลลัพธ์ของการศึกษา ผลการวิจัย: เรารวม RCTs 37 ฉบับ (มีผู้เข้าร่วม 2766 คน), 26 ฉบับเผยแพร่ตั้งแต่การอัปเดตครั้งก่อน กลุ่ม CS ที่ได้รับการประเมินมากที่สุด 8 ฉบับตรวจสอบ CS แต่ละบุคคล อายุเฉลี่ยของผู้เข้าร่วมคือ 79.7 ปี การศึกษา 16 ฉบับรวมผู้เข้าร่วมที่อาศัยอยู่ในบ้านพักคนชราหรือโรงพยาบาล คุณภาพการศึกษาแสดงให้เห็นการปรับปรุงตั้งแต่การทบทวนครั้งก่อน โดยมีบางประเด็นที่มีความเสี่ยงสูงที่จะเกิดอคติ ผู้ประเมินได้รับการปกปิดอย่างชัดเจนต่อการจัดสรรการรักษาในการศึกษาส่วนใหญ่ (81%) และการศึกษาส่วนใหญ่ (81%) รายงานการใช้คู่มือการรักษาโดยผู้ที่ให้การรักษา อย่างไรก็ตาม ในการศึกษาจำนวนมาก (59%) เราไม่พบรายละเอียดในทุกแง่มุมของขั้นตอนการสุ่ม ทำให้เราให้คะแนนความเสี่ยงของอคติในการคัดเลือกว่าไม่ชัดเจน เราป้อนข้อมูลในการวิเคราะห์อภิมานจากการศึกษา 36 ฉบับ (ผู้เข้าร่วม 2704 คน CS: 1432, กลุ่มควบคุม: 1272) การวิเคราะห์เบื้องต้นเกี่ยวกับการเปลี่ยนแปลงที่เห็นได้ชัดทันทีหลังจากระยะเวลาการรักษา (ความยาวเฉลี่ย 10 สัปดาห์ ช่วง 4 ถึง 52 สัปดาห์) มีเพียงการศึกษา 8 ฉบับเท่านั้นที่ให้ข้อมูลที่ช่วยให้สามารถประเมินได้ว่าผลกระทบนั้นยังคงอยู่หรือไม่ (การศึกษา 4 ฉบับ ติดตามผล 6 ถึง 12 สัปดาห์; 4 ฉบับ ติดตามผล 8 ถึง 12 เดือน) ไม่มีรายงานผลกระทบด้านลบ โดยรวมแล้ว เราพบหลักฐานที่มีคุณภาพปานกลางว่ามีประโยชน์เล็กน้อยในการรับรู้ที่เกี่ยวข้องกับ CS (ความแตกต่างของค่าเฉลี่ยมาตรฐาน (SMD) 0.40, 95% CI 0.25 ถึง 0.55) ในการศึกษา 25 ฉบับ ซึ่งมีผู้เข้าร่วม 1893 คน ซึ่งรายงานการทดสอบ MMSE (Mini‐Mental State Examination) ที่ใช้กันอย่างแพร่หลายสำหรับการทำงานของการรับรู้ในภาวะสมองเสื่อม มีหลักฐานที่มีคุณภาพปานกลางของความแตกต่างที่สำคัญทางคลินิก 1.99 คะแนนระหว่าง CS และกลุ่มควบคุม (95% CI: 1.24, 2.74) ในการวิเคราะห์ระดับทุติยภูมิ ซึ่งมีขนาดตัวอย่างทั้งหมดน้อยลง ตรวจสอบความแตกต่างอีกครั้งระหว่าง CS และกลุ่มควบคุมเกี่ยวกับการเปลี่ยนแปลงทันทีหลังจากช่วงแทรกแซง เราพบหลักฐานคุณภาพปานกลางของการปรับปรุงเล็กน้อยใน QoL ที่รายงานด้วยตนเอง (การศึกษา 18 ฉบับ ผู้เข้าร่วม 1584 คน; SMD: 0.25 [95% CI: 0.07, 0.42]) เช่นเดียวกับการให้คะแนน QoL ที่จัดทำโดยตัวแทน (เจ้าหน้าที่หรือผู้ดูแล) เราพบหลักฐานคุณภาพสูงสำหรับการปรับปรุงที่เกี่ยวข้องทางคลินิกในการให้คะแนนการสื่อสารและปฏิสัมพันธ์ทางสังคมของพนักงาน/ผู้สัมภาษณ์ (การศึกษา 5 ฉบับ ผู้เข้าร่วม 702 คน; SMD: 0.53 [95% CI: 0.36, 0.70]) และมีประโยชน์เล็กน้อยวัดโดยเครื่องมือกิจกรรมในชีวิตประจำวัน (instrumental Activities of Daily Living) อารมณ์ซึมเศร้าที่รายงานด้วยตนเอง ความวิตกกังวลที่ประเมินโดยเจ้าหน้าที่/ผู้สัมภาษณ์ และมาตราส่วนการให้คะแนนพฤติกรรมทั่วไป เราพบหลักฐานคุณภาพปานกลางสำหรับการปรับปรุงเล็กน้อยในพฤติกรรมที่ท้าทายและในกิจกรรมพื้นฐานของชีวิตประจำวัน และหลักฐานคุณภาพต่ำสำหรับการปรับปรุงเล็กน้อยในอารมณ์ซึมเศร้าที่ประเมินโดยพนักงาน/ผู้สัมภาษณ์ การศึกษาบางฉบับรายงานผลลัพธ์ที่หลากหลายสำหรับผู้ดูแลในครอบครัว เราพบหลักฐานที่มีคุณภาพปานกลางว่า CS โดยรวมสร้างความแตกต่างเล็กน้อยหรือไม่มีเลยต่ออารมณ์หรือความวิตกกังวลของผู้ดูแล เราพบความไม่สอดคล้องกันในระดับสูงระหว่างการศึกษาที่เกี่ยวข้องกับทั้งผลลัพธ์ทางปัญญาและ QoL ในการวิเคราะห์กลุ่มย่อยเชิงสำรวจ เราไม่พบผลกระทบของวิธีการ (กลุ่มเทียบกับรายบุคคล) หรือการศึกษากลุ่ม สถานที่ (ชุมชนกับสถานดูแล) จำนวนเซสชันทั้งหมดของกลุ่มหรือประเภทของเงื่อนไขการควบคุม (การรักษาตามปกติเทียบกับ ตัวควบคุมที่ใช้งานอยู่) อย่างไรก็ตาม เราพบว่าการปรับปรุงความรู้ความเข้าใจมีมากขึ้นเมื่อเซสชันแบบกลุ่มมีบ่อยขึ้น (2 ครั้งต่อสัปดาห์หรือมากกว่านั้นเมื่อเทียบกับสัปดาห์ละครั้ง) และความรุนแรงของภาวะสมองเสื่อมโดยเฉลี่ยในกลุ่มผู้เข้าร่วมในช่วงเริ่มต้นของการแทรกแซงคือ 'เล็กน้อย' แทนที่จะเป็น 'ปานกลาง' ความไม่สมดุลของจำนวนการศึกษาและผู้เข้าร่วมระหว่างกลุ่มย่อยและความไม่สอดคล้องกันที่เหลืออยู่ ทำให้ต้องตีความการค้นพบเชิงสำรวจเหล่านี้อย่างระมัดระวัง ข้อสรุปของผู้วิจัย: ในการทบทวนฉบับปรับปรุงนี้ ขณะนี้มีหลักฐานที่กว้างขวางมากขึ้น เราได้พบประโยชน์ทางปัญญาในระยะสั้นเล็กน้อยอีกครั้งสำหรับผู้ที่มีภาวะสมองเสื่อมระดับเล็กน้อยถึงปานกลางที่เข้าร่วมโปรแกรม CS จากการศึกษาจำนวนน้อย เรายังพบการปรับปรุงที่เกี่ยวข้องทางคลินิกในการสื่อสารและปฏิสัมพันธ์ทางสังคม และผลประโยชน์เล็กน้อยในผลลัพธ์ต่างๆ รวมถึง QoL อารมณ์และพฤติกรรมที่ท้าทาย มีการศึกษาค่อนข้างน้อยเกี่ยวกับ CS ส่วนบุคคล และจำเป็นต้องมีการวิจัยเพิ่มเติมเพื่อระบุประสิทธิผลของวิธีการจัดส่งที่แตกต่างกัน (รวมถึงแบบดิจิทัลและระยะไกล รายบุคคลและกลุ่ม) และของโปรแกรมที่มีหลายองค์ประกอบ เราพบว่าความถี่ของกิจกรรมกลุ่มและระดับความรุนแรงของภาวะสมองเสื่อมอาจส่งผลต่อผลลัพธ์ของ CS และควรศึกษาประเด็นเหล่านี้เพิ่มเติม ยังคงมีช่องว่างของหลักฐานที่เกี่ยวข้องกับผลประโยชน์ที่เป็นไปได้ของโปรแกรม CS ระยะยาวและความสำคัญทางคลินิก.
پیشینه: تحریک شناختی (cognitive stimulation; CS)، مداخلهای است برای افراد مبتلا به دمانس، و شامل طیف وسیعی از فعالیتهای لذتبخشی است که معمولا در یک محیط اجتماعی، مانند یک گروه کوچک، خدمات تحریک تفکر، تمرکز و حافظه را ارائه میدهد. CS با تمرکز گسترده و عناصر اجتماعی خود از رویکردهای دیگری مانند آموزش شناختی و توانبخشی شناختی متمایز میشود و هدف آن بهبود حوزههایی مانند کیفیت زندگی (QoL)، خلقوخو و همچنین عملکرد شناختی فرد بیمار است. استفاده از این روش در دستورالعملهای بالینی مختلف توصیه شده و بهطور گستردهای در سطح بینالمللی اجرا میشود، هرچند در مورد روشهای مختلف ارائه و اهمیت بالینی هرگونه مزیت حاصل از آن هنوز هم سوالاتی وجود دارد. برای روشن شدن اثربخشی آن و ارائه توصیههای عملی بر پایه شواهد معتبر، انجام یک مرور سیستماتیک درباره CS مهم است. این مرور آخرین بار در سال 2012 بهروز شد. اهداف: ارزیابی شواهد مربوط به اثربخشی CS در افراد مبتلا به دمانس، از جمله هرگونه تاثیرات منفی بر شناخت و دیگر پیامدهای مرتبط، و تا جایی که امکانپذیر است باید در اجرای آن، تفاوتها در نظر گرفته شود. روشهای جستوجو: کارآزماییها را از طریق جستوجو در پایگاه ثبت تخصصی گروه دمانس و بهبود شناختی در کاکرین شناسایی کردیم، آخرین جستوجو در 3 مارچ سال 2022 انجام شد. از اصطلاحات جستوجوی زیر استفاده کردیم: تحریک شناختی، آگاهی از واقعیت، حافظه درمانی، گروههای حافظه، حمایت از حافظه، تحریک حافظه، تحریک کلی، تحریک روانی شناختی. جستوجوهای تکمیلی را در تعدادی از بانکهای اطلاعاتی اصلی مراقبت سلامت و پایگاههای ثبت کارآزمایی انجام دادیم تا اطمینان حاصل کنیم که جستوجو بهروز و جامع است. معیارهای انتخاب: همه کارآزماییهای تصادفیسازی و کنترل شده (randomised controlled trials; RCTs) را در رابطه با بررسی تاثیر CS در درمان دمانس وارد کردیم که در مجلات با داوری همتا (peer review) به زبان انگلیسی منتشر شده، و شامل معیار تغییرات شناختی بودند. گردآوری و تجزیهوتحلیل دادهها: از پروسیجرهای استاندارد روششناسی (methodology) مورد نظر کاکرین استفاده کردیم. از آنجایی که CS یک مداخله روانیاجتماعی است، انتظار نداشتیم کسانی که CS را دریافت کردند یا کسانی که آن را به شرکتکنندگان ارائه دادند نسبت به ماهیت مداخله کورسازی شوند. در صورت لزوم، با نویسندگان مطالعه تماس گرفته و اطلاعاتی را که در مقالات ارائه نشده بودند، درخواست کردیم. در صورت لزوم، تجزیهوتحلیل زیر گروه را بر اساس روش (فردی در برابر گروهی)، تعداد جلسات و دفعات، محیط (جامعه در برابر خانه مراقبت)، نوع شرایط کنترل و شدت دمانس انجام دادیم. از روشهای درجهبندی توصیه، ارزیابی، توسعه و ارزشیابی (Grading of Recommendations Assessment, Development and Evaluation; GRADE) برای ارزیابی کیفیت کلی شواهد برای هر پیامد استفاده کردیم. نتایج اصلی: تعداد 37 RCT (با 2766 شرکتکننده) را در این مرور گنجاندیم، 26 مورد از زمان نسخه بهروز شده قبلی منتشر شدند. اکثرا CS گروهی را ارزیابی کردند؛ در هشت مورد هم CS فردی مورد بررسی قرار گرفت. میانه (median) سنی شرکتکنندگان 79.7 سال بود. شانزده مطالعه شامل شرکتکنندگان ساکن در خانههای مراقبت یا بیمارستانها بودند. سطح کیفیت مطالعه نسبت به مرور قبلی ارتقا یافت، با حیطههای اندکی که خطر بالای سوگیری (bias) داشت. ارزیابان به وضوح نسبت به تخصیص درمان در اکثر مطالعات (81%) کور شده بودند، و بیشتر مطالعات (81%) استفاده از کتابچه راهنمای درمان را توسط کسانی که مداخله را ارائه دادند گزارش کردند. با این حال، در تعداد قابلتوجهی از مطالعات (59%)، نتوانستیم جزئیات مربوط به تمام جنبههای پروسیجرهای تصادفیسازی را پیدا کنیم، که باعث شد خطر سوگیری انتخاب را نامشخص ارزیابی کنیم. دادههای 36 مطالعه را در متاآنالیزها وارد کردیم (2704 شرکتکننده؛ CS: 1432، کنترل: 1272). آنالیز اولیه روی تغییرات مشهود بلافاصله پس از دوره درمان انجام شد (میانه (median): 10 هفته، 4 تا 52 هفته). فقط هشت مطالعه دادههایی را ارائه دادند که امکان ارزیابی تاثیرات بعدی را فراهم کردند (چهار مورد در پیگیری 6 تا 12 هفته، چهار مورد در پیگیری 8 تا 12 ماه). تاثیرات منفی گزارش نشدند. بهطور کلی، شواهدی را با کیفیت متوسط حاکی از یک مزیت کوچک در شناخت مرتبط با CS به دست آوردیم (تفاوت میانگین استاندارد شده (SMD): 0.40؛ 95% CI؛ 0.25 تا 0.55). در 25 مطالعه، با 1893 شرکتکننده، که استفاده از تست پُرکاربرد MMSE (آزمون کوتاه وضعیت ذهنی (Mini‐Mental State Examination)) را برای عملکرد شناختی در دمانس گزارش کردند، شواهدی با کیفیت متوسط حاکی از تفاوت بالینی مهم 1.99 امتیازی بین CS و گروه کنترل وجود داشت (95% CI؛ 1.24 تا 2.74). در آنالیزهای ثانویه، با حجم نمونه کلی کمتر، مجددا با بررسی تفاوت بین CS و کنترلها از لحاظ بروز تغییرات بلافاصله پس از مداخله، شواهدی را با کیفیت متوسط حاکی از بهبود جزئی در QoL گزارش شده توسط خود بیمار یافتیم (18 مطالعه، 1584 شرکتکننده؛ SMD: 0.25؛ [95% CI؛ 0.07 تا 0.42]) همچنین در رتبهبندیهای QoL بر اساس پراکسیها (کارکنان یا مراقبان) این مزیت مداخله دیده شد. شواهدی را با کیفیت بالا برای بهبودهای مرتبط بالینی در رتبهبندی کارکنان/مصاحبهگر از ارتباطات و اثر متقابل (interaction) اجتماعی (5 مطالعه، 702 شرکتکننده؛ SMD: 0.53؛ [95% CI؛ 0.36، 0.70]) و برای مزایای جزئی در فعالیتهای ابزاری زندگی روزانه (instrumental)، خلقوخوی افسرده بر اساس گزارش خود فرد، اضطراب رتبهبندی شده توسط کارکنان/مصاحبهگر و مقیاسهای رتبهبندی رفتار کلی فرد پیدا کردیم. شواهدی با کیفیت متوسط برای بهبودهای جزئی در رفتار و در فعالیتهای زندگی پایه (basic) روزانه و شواهدی با کیفیت پائین برای بهبود جزئی در خلقوخوی افسرده رتبهبندی شده توسط کارکنان/مصاحبهگر پیدا شد. مطالعات معدودی طیف وسیعی را از پیامدها برای مراقبان خانواده گزارش کردند. شواهدی را با کیفیت متوسط پیدا کردیم که نشان میدهد CS کلی تفاوتی اندک یا عدم تفاوت را در خلقوخو یا اضطراب مراقبین بر جای میگذارد. سطح بالایی را از ناهمگونی بین مطالعات را در رابطه با پیامدهای شناختی و QoL یافتیم. در آنالیزهای زیرگروه اکتشافی، تاثیر روش (گروهی در برابر فردی) یا، برای مطالعات گروهی، محیط (جامعه در برابر خانه مراقبت)، تعداد کل جلسات گروهی یا نوع شرایط کنترل (درمان طبق معمول در برابر کنترلهای فعال) را شناسایی نکردیم. با این حال، متوجه شدیم در جایی که جلسات گروهی به دفعات بیشتری برگزار شد (دو بار در هفته یا بیشتر در برابر یک بار در هفته) و جایی که میانگین شدت دمانس میان شرکتکنندگان در شروع مداخله به جای «متوسط»، در سطح «خفیف» بود، بهبود شناخت بیشتر رخ داد. عدم تعادل در تعداد مطالعات و شرکتکنندگان بین زیرگروهها و ناهمگونی باقیمانده، نیازمند این است که این یافتههای اکتشافی با احتیاط تفسیر شوند. نتیجهگیریهای نویسندگان: در این مرور بهروز شده، اکنون با یک مجموعه شواهد بسیار گستردهتر، باز هم مزایای شناختی کوچک و کوتاهمدت را برای افراد مبتلا به دمانس خفیف تا متوسط که در برنامههای CS شرکت میکنند، شناسایی کردهایم. از تعداد کمتری از مطالعات، همچنین بهبودهای مرتبط بالینی در ارتباطات و اثر متقابل (interaction) اجتماعی و مزایای جزئی را در طیف وسیعی از پیامدها از جمله QoL، خلقوخو و رفتار چالش برانگیز، به دست آوردهایم. مطالعات نسبتا کمی در مورد CS فردی وجود دارد، انجام پژوهشهای بیشتری برای تشریح اثربخشی روشهای مختلف ارائه (از جمله دیجیتال و از راه دور، فردی و گروهی) و برنامههای چند جزئی مورد نیاز است. به این نتیجه رسیدیم که فراوانی جلسات گروهی و سطح شدت دمانس ممکن است بر پیامدهای CS تاثیر بگذارند، و این جنبهها باید بیشتر مورد مطالعه قرار گیرند. در رابطه با مزایای بالقوه برنامههای طولانیمدتتر CS و اهمیت بالینی آنها شکاف شواهد وجود دارد.
Contexte: La stimulation cognitive (SC) est une intervention destinée aux personnes atteintes de démence qui propose une série d'activités agréables stimulant de manière générale la pensée, la concentration et la mémoire, généralement dans un cadre social comme un petit groupe. La SC se distingue d'autres approches telles que l'entraînement cognitif et la rééducation cognitive par son orientation générale et ses éléments sociaux, visant à améliorer des domaines tels que la qualité de vie (QV) et l'humeur, ainsi que la fonction cognitive. Préconisée dans diverses recommandations et largement mise en œuvre au niveau international, des questions subsistent quant aux différents modes d'administration et à l'importance clinique des bénéfices éventuels. Une étude systématique de la SC est importante pour clarifier son efficacité et établir des recommandations pratiques sur des données probantes solides. Cette revue a été mise à jour pour la dernière fois en 2012.
Objectifs: Évaluer les données probantes de l'efficacité de la SC pour les personnes atteintes de démence, y compris les effets négatifs, sur la cognition et d'autres critères de jugement pertinents, en tenant compte si possible des différences dans sa mise en œuvre. STRATÉGIE DE RECHERCHE DOCUMENTAIRE: Nous avons identifié des essais à partir d'une recherche dans le registre spécialisé du groupe Cochrane sur la démence et les autres troubles cognitifs, consulté pour la dernière fois le 3 mars 2022. Nous avons utilisé les termes de recherche suivants: stimulation cognitive, orientation vers la réalité, thérapie de la mémoire, groupes de mémoire, soutien de la mémoire, stimulation de la mémoire, stimulation globale, psychostimulation cognitive. Nous avons effectué des recherches supplémentaires dans un certain nombre de grandes bases de données sur les soins de santé et de registres d'essais pour nous assurer que la recherche était à jour et complète. CRITÈRES DE SÉLECTION: Nous avons inclus tous les essais contrôlés randomisés (ECR) de la SC pour la démence publiés dans des revues avec comité de lecture en langue anglaise et incorporant une mesure du changement cognitif. RECUEIL ET ANALYSE DES DONNÉES: Nous avons suivi les procédures méthodologiques standard prévues par Cochrane. Comme la SC est une intervention psychosociale, nous ne nous attendions pas à ce que les personnes recevant ou délivrant la SC soient prévenues à la nature de l'intervention. Quand cela était nécessaire, nous avons contacté les auteurs des études pour leur demander des données non fournies dans les articles. Le cas échéant, nous avons effectué une analyse en sous‐groupe en fonction de la modalité (individuelle ou de groupe), du nombre de séances et de leur fréquence, du contexte (communauté ou établissements de soins), du type de condition de contrôle et de la gravité de la démence. Nous avons utilisé les méthodes GRADE pour évaluer la qualité globale des données probantes pour chaque critère de jugement. RÉSULTATS PRINCIPAUX: Nous avons inclus 37 ECR (avec 2766 participants), dont 26 publiés depuis la mise à jour précédente. La plupart ont évalué des groupes de SC ; huit ont examiné la SC individuelle. L'âge médian des participants était de 79,7 ans. Seize études ont inclus des participants résidant dans des maisons de soins ou des hôpitaux. La qualité des études a montré des signes d'amélioration depuis la revue précédente, avec peu d’éléments à risque de biais élevé. Les évaluateurs étaient clairement en aveugle par rapport à l'allocation des traitements dans la plupart des études (81%) et la plupart des études (81%) ont rapporté l'utilisation d'un manuel de traitement par ceux qui délivraient l'intervention. Cependant, dans un nombre important d'études (59 %), nous n'avons pas pu trouver de détails sur tous les aspects des procédures de randomisation, ce qui nous a conduits à classer le risque de biais de sélection comme incertain. Nous avons saisi dans les méta‐analyses les données de 36 études (2704 participants ; SC : 1432, contrôles : 1272). L'analyse principale a porté sur les changements manifestes immédiatement après la période de traitement (durée médiane de 10 semaines ; intervalle de 4 à 52 semaines). Seules huit études ont fourni des données permettant d'évaluer si les effets se sont maintenus par la suite (quatre avec un suivi de 6 à 12 semaines ; quatre avec un suivi de 8 à 12 mois). Les effets négatifs n’ont pas été rapportés. Dans l'ensemble, nous avons trouvé des données probantes de qualité modérée d'un léger bénéfice sur la cognition associé à la SC (différence de moyennes standardisée (DMS) 0,40, IC à 95 % 0,25 à 0,55). Dans les 25 études, avec 1893 participants, qui ont rapporté le test MMSE (Mini‐Mental State Examination) largement utilisé pour la fonction cognitive dans la démence, il y avait des données probantes de qualité modérée d'une différence cliniquement importante de 1,99 points entre les SC et les contrôles (IC à 95%: 1.24, 2.74). Dans les analyses secondaires, avec des tailles d'échantillon totales plus petites, évaluant à nouveau la différence entre les SC et les contrôles sur les changements immédiatement après la période d'intervention, nous avons trouvé des données probantes de qualité modérée d'une légère amélioration de la qualité de vie autodéclarée (18 études, 1584 participants ; DMS : 0,25 [IC à 95 % : 0,07, 0,42]) ainsi que dans les évaluations de la qualité de vie effectuées par des mandataires (personnel ou soignants). Nous avons trouvé des données probantes de haute qualité pour des améliorations cliniquement pertinentes dans les évaluations du personnel/intervieweur de la communication et de l'interaction sociale (5 études, 702 participants ; DMS : 0,53 [IC à 95 %: 0,36, 0,70]) et pour de légers bénéfices dans l’échelle d'évaluation instrumental Activities of Daily Living (activités de la vie quotidienne), l'humeur dépressive autodéclarée, l'anxiété évaluée par le personnel/interviewer et les échelles d'évaluation du comportement général. Nous avons trouvé des données probantes de qualité modérée pour de légères améliorations dans le comportement problématique et dans les activités de base de la vie quotidienne et des données probantes de faible qualité pour une légère amélioration de l'humeur dépressive évaluée par le personnel/interviewer. Quelques études ont rapporté une série de critères de jugement pour les aidants familiaux. Nous avons trouvé des données probantes de qualité modérée suggérant que, dans l'ensemble, la SC a fait peu ou pas de différence sur l'humeur ou l'anxiété des soignants. Nous avons constaté un niveau élevé d'incohérence entre les études en ce qui concerne les critères de jugement cognitifs et la qualité de vie. Dans les analyses exploratoires de sous‐groupes, nous n'avons pas identifié d'effet de la modalité (groupe ou individu) ou, pour les études de groupe, du cadre (communauté ou établissements de soins), du nombre total de sessions de groupe ou du type de condition de contrôle (traitement habituel ou contrôles actifs). Cependant, nous avons constaté que les améliorations cognitives étaient plus importantes lorsque les sessions de groupe étaient plus fréquentes (deux fois par semaine ou plus contre une fois par semaine) et lorsque la gravité moyenne de la démence parmi les participants au début de l'intervention était « légère » plutôt que « modérée ». Le déséquilibre dans le nombre d'études et de participants entre les sous‐groupes et l'incohérence résiduelle exigent que ces résultats exploratoires soient interprétés avec prudence.
Conclusions des auteurs: Dans cette mise à jour de la revue, qui s'appuie désormais sur une base beaucoup plus vaste de données probantes, nous avons à nouveau identifié de petits bénéfices cognitifs à court terme pour les personnes atteintes de démence légère à modérée qui participent à des programmes de stimulation cognitive. Dans un plus petit nombre d'études, nous avons également constaté des améliorations cliniquement significatives en matière de communication et d'interaction sociale, ainsi que de légers bénéfices dans une série de critères de jugement, notamment la qualité de vie, l'humeur et les comportements problématiques. Il existe relativement peu d'études sur la stimulation cognitive individuelle, et des recherches supplémentaires sont nécessaires pour déterminer l'efficacité des différentes méthodes d'enseignement (notamment numériques et à distance, individuelles et collectives) et des programmes à composantes multiples. Nous avons identifié que la fréquence des sessions de groupe et le niveau de sévérité de la démence pourraient influencer les critères de jugement de la SC, et ces aspects devraient être étudiés de manière approfondie. Il existe un manque de données probantes sur les bénéfices potentiels des programmes de SC à long terme et leur pertinence clinique.
Antecedentes: La estimulación cognitiva (EC) es una intervención para personas con demencia que ofrece una serie de actividades amenas que estimulan de forma general el pensamiento, la concentración y la memoria, normalmente en un contexto social, como un pequeño grupo. La EC se distingue de otros enfoques, como el entrenamiento cognitivo y la rehabilitación cognitiva, por su enfoque amplio y sus elementos sociales, cuyo objetivo es mejorar aspectos como la calidad de vida (CdV) y el estado de ánimo, además de la función cognitiva. Aunque se recomienda en varias guías y se aplica ampliamente a escala internacional, sigue habiendo dudas sobre las distintas formas de administración y la importancia clínica de sus posibles efectos beneficiosos. Es importante elaborar una revisión sistemática de la EC para aclarar su efectividad y basar las recomendaciones prácticas en evidencia sólida. Esta revisión se actualizó por última vez en 2012.
Objetivos: Evaluar la evidencia de la efectividad de la EC para las personas con demencia, incluidos los efectos negativos, sobre la cognición y otros desenlaces relevantes, teniendo en cuenta, en la medida de lo posible, las diferencias en su aplicación. MÉTODOS DE BÚSQUEDA: Se identificaron ensayos a partir de una búsqueda en el Registro especializado del Grupo Cochrane de Demencia y trastornos cognitivos (Cochrane Dementia and Cognitive Improvement Group), última búsqueda realizada el 3 de marzo de 2022. Se utilizaron los términos de búsqueda: cognitive stimulation, reality orientation, memory therapy, memory groups, memory support, memory stimulation, global stimulation, cognitive psychostimulation. Se realizaron búsquedas complementarias en varias de las principales bases de datos de asistencia sanitaria y registros de ensayos para garantizar que la búsqueda estuviera actualizada y fuera exhaustiva. CRITERIOS DE SELECCIÓN: Se incluyeron todos los ensayos controlados aleatorizados (ECA) de la EC para la demencia publicados en revistas de revisión por pares en inglés que incorporaran una medida de cambio cognitivo. OBTENCIÓN Y ANÁLISIS DE LOS DATOS: Se utilizaron los procedimientos metodológicos estándar previstos por Cochrane. Como la EC es una intervención psicosocial, no se esperaba que se ocultara la naturaleza de la intervención a quienes recibían o administraban la EC. Cuando fue necesario, se estableció contacto con los autores de los estudios para solicitar datos no proporcionados en los artículos. Cuando fue apropiado, se realizaron análisis de subgrupos según la modalidad (individual versus grupal), el número de sesiones y la frecuencia, el contexto (comunitario versus residencial), el tipo de condición de control y la gravedad de la demencia. Se utilizó el método GRADE para evaluar la calidad general de la evidencia para cada desenlace.
Resultados principales: Se incluyeron 37 ECA (con 2766 participantes), 26 publicados desde la actualización anterior. La mayoría evaluaron la EC grupal; ocho examinaron la EC individual. La mediana de edad de los participantes fue 79,7 años. Dieciséis estudios incluyeron participantes internos en residencias u hospitales. La calidad de los estudios mostró indicios de mejoría desde la revisión anterior, con pocas áreas de alto riesgo de sesgo. La mayoría de estudios (81%) ocultaron la asignación al tratamiento a los evaluadores y la mayoría de los estudios (81%) informaron de que quienes administraron la intervención utilizaron un manual de tratamiento. Sin embargo, en un número considerable de estudios (59%), no se pudieron encontrar detalles sobre todos los aspectos de los procedimientos de asignación al azar, lo que hizo que el riesgo de sesgo de selección se considerara incierto. En los metanálisis se introdujeron los datos de 36 estudios (2704 participantes; EC: 1432, controles: 1272). El análisis principal se centró en los cambios evidentes inmediatamente después del periodo de tratamiento (duración media de 10 semanas; intervalo: 4 a 52 semanas). Solo ocho estudios proporcionaron datos que permitieron evaluar si los efectos se mantenían posteriormente (cuatro con un seguimiento de 6 a 12 semanas; cuatro con un seguimiento de 8 a 12 meses). No se notificaron efectos negativos. En general, se encontró evidencia de calidad moderada de un pequeño efecto beneficioso en la cognición asociado con la EC (diferencia de medias estandarizada [DME] 0,40; IC del 95%: 0,25 a 0,55). En los 25 estudios, con 1893 participantes, que informaron sobre la prueba MMSE (Mini‐Mental State Examination) ampliamente utilizada para la función cognitiva en la demencia, hubo evidencia de calidad moderada de una diferencia clínicamente importante de 1,99 puntos entre los que recibieron EC y los controles (IC del 95%: 1,24 a 2,74). En los análisis secundarios, con tamaños muestrales totales más pequeños, que examinaron de nuevo la diferencia entre la EC y los controles sobre los cambios inmediatamente después del periodo de intervención, se encontró evidencia de calidad moderada de una ligera mejoría en la CdV autoinformada (18 estudios, 1584 participantes; DME: 0,25 [IC del 95%: 0,07 a 0,42]), así como en las valoraciones de la CdV realizadas por sus representantes (personal o cuidadores). Se encontró evidencia de calidad alta de mejorías clínicamente relevantes en las calificaciones del personal/encuestadores relacionadas con la comunicación y la interacción social (cinco estudios, 702 participantes; DME: 0,53 [IC del 95%: 0,36 a 0,70]) y de ligeros efectos beneficiosos en las escalas de calificación instrumentales Activities of Daily Living (actividades cotidianas), estado de ánimo depresivo autoinformado, ansiedad calificada por el personal/encuestadores y comportamiento general. Se encontró evidencia de calidad moderada de mejorías leves en el comportamiento desafiante y en la Activities of Daily Living y evidencia de calidad baja de una mejoría leve en el estado de ánimo depresivo calificado por el personal/encuestadores. Unos pocos estudios informaron sobre una serie de desenlaces relacionados con los cuidadores familiares. Se encontró evidencia de calidad moderada de que, en general, la EC tuvo poca o ninguna repercusión en el estado de ánimo o la ansiedad de los cuidadores. Se encontró un alto nivel de inconsistencia entre los estudios en relación con los desenlaces cognitivos y la CdV. En los análisis exploratorios de subgrupos, no se identificó un efecto de la modalidad (grupal versus individual) o, en los estudios por conglomerados, del contexto (comunidad versus residencial), el número total de sesiones grupales ni el tipo de control (tratamiento habitual versus controles activos). Sin embargo, se observó que las mejorías en la cognición fueron mayores cuando las sesiones grupales eran más frecuentes (dos veces por semana o más versus una vez por semana) y cuando la gravedad media de la demencia entre los participantes al inicio de la intervención era "leve" en lugar de "moderada". El desequilibrio en el número de estudios y participantes entre los subgrupos y la inconsistencia residual requieren que estos hallazgos exploratorios se interpreten con cautela.
Conclusiones de los autores: En esta revisión actualizada, ahora con una base de evidencia mucho más grande, se han vuelto a identificar pequeños efectos beneficiosos cognitivos a corto plazo en las personas con demencia leve a moderada que participan en programas de EC. A partir de un número menor de estudios, también se han encontrado mejorías clínicamente relevantes en la comunicación y la interacción social y ligeros efectos beneficiosos en una serie de desenlaces que incluyen la CdV, el estado de ánimo y el comportamiento desafiante. Existen relativamente pocos estudios sobre la EC individual y es necesario seguir investigando para determinar la efectividad de los distintos métodos de administración (digital y a distancia, individual y grupal) y de los programas multicomponentes. Se ha identificado que la frecuencia de las sesiones grupales y el nivel de gravedad de la demencia podrían influir en los desenlaces de la EC y estos aspectos se deben estudiar más a fondo. Aún falta de evidencia en relación con los posibles efectos beneficiosos de los programas de EC a largo plazo y su importancia clínica.
Copyright © 2023 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Conflict of interest statement
The authors have produced various training materials in dementia care, including cognitive stimulation therapy manuals, in order to disseminate research findings to care workers, family caregivers and others. Royalties for the manuals are received by the International Cognitive Stimulation Therapy Centre, based at University College London. AS receives fees for providing training in cognitive stimulation approaches.
Figures
















































































Update of
References
References to studies included in this review
Ali 2021 {published data only}
Alvares‐Pereira 2021 {published data only}
Baldelli 1993 {published data only}
-
- Baldelli MV, Pirani A, Motta M, Abati E, Mariani E, Manzi V. Effects of reality orientation therapy on elderly patients in the community. Archives of Gerontology and Geriatrics 1993a;17(3):211-8. - PubMed
Baldelli 2002 {published data only}
-
- Baldelli MV, Boiardi R, Fabbo A, Pradelli JM, Neri M. The role of reality orientation therapy in restorative care of elderly patients with dementia plus stroke in the subacute nursing home setting. Archives of Gerontology and Geriatrics 2002;35 Suppl 8:15-22. - PubMed
Bottino 2005 {published data only}
-
- Bottino CMC, Carvalho IAM, Alvarez AM, Avila R, Zukauskas PR, Bustamante SEZ, et al. Cognitive rehabilitation combined with drug treatment in Alzheimer's disease patients: a pilot study. Clinical Rehabilitation 2005;19:861-9. - PubMed
Breuil 1994 {published data only}
-
- Breuil V, De Rotrou J, Forette F, Tortrat D, Ganansia Ganem A, Frambourt A, et al. Cognitive stimulation of patients with dementia: preliminary results. International Journal of Geriatric Psychiatry 1994;9(3):211-7.
Buschert 2011 {published data only}
-
- Buschert VC, Friese U, Teipel SJ, Schneider P, Merensky W, Rujescu D, et al. Effects of a newly developed cognitive intervention in amnestic mild cognitive impairment and mild Alzheimer's disease: a pilot study. Journal of Alzheimer's Disease 2011;25:679-94. [DOI: 10.3233/JAD-2011-100999] - DOI - PubMed
Capotosto 2017 {published data only}
-
- Capotosto E, Belacchi C, Gardini S, Faggian S, Piras F, Mantoan V, et al. Cognitive stimulation therapy in the Italian context: its efficacy in cognitive and non-cognitive measures in older adults with dementia. International Journal of Geriatric Psychiatry 2017;32(3):331-40. [DOI: 10.1002/gps.4521] - DOI - PubMed
Carbone 2021 {published and unpublished data}
-
- Carbone E, Gardini S, Pastore M, Piras F, Vincenzi, M, Borella E. Cognitive Stimulation Therapy (CST) for older adults with mild-to-moderate dementia in Italy: effects on cognitive functioning and on emotional and neuropsychiatric symptoms. Journals of Gerontology Series B: Psychological Sciences & Social Sciences 2021;76:1700-10. [DOI: 10.1093/geronb/gbab007] - DOI - PubMed
Chapman 2004 {published data only}
-
- Chapman SB, Weiner MF, Rackley A, Hynan LS, Zientz J. Effects of cognitive-communication stimulation for Alzheimer's disease patients treated with donepezil. Journal of Speech, Language, and Hearing Research 2004;47(5):1149-63. - PubMed
Cheung 2019 {published data only}
Coen 2011 {published data only}
-
- Coen RF, Flynn B, Rigney E, O'Connor E, Fitzgerald L, Murray C, et al. Efficacy of a cognitive stimulation therapy programme for people with dementia. Irish Journal of Psychological Medicine 2011;28(3):145-7. - PubMed
Cove 2014 {published data only}
-
- Cove J, Jacobi N, Donovan H, Orrell M, Stott J, Spector A. Effectiveness of weekly cognitive stimulation therapy for people with dementia and the additional impact of enhancing cognitive stimulation therapy with a carer training program. Clinical Interventions in Aging 2014;9:2143-50. [DOI: ] - PMC - PubMed
Gibbor 2020b {published data only}
-
- Gibbor L, Forde L, Yates L, Orfanos S, Komodromos C, Page H, et al. A feasibility randomised control trial of individual cognitive stimulation therapy for dementia: impact on cognition, quality of life and positive psychology. Aging & Mental Health 2020;25:999-1007. [DOI: 10.1080/13607863.2020.1747048] - DOI - PubMed
Graessel 2011 {published data only}
-
- Luttenberger K, Donath C, Uter W, Graessel E. Effects of multimodal nondrug therapy on dementia symptoms and need for care in nursing home residents with degenerative dementia: a randomized-controlled study with 6-month follow-up. Journal of the American Geriatrics Society 2012;60(5):830-40. [DOI: 10.1111/j.1532-5415.2012.03938.x] - DOI - PubMed
Juarez‐Cedillo 2020 {published data only}
-
- Juarez-Cedillo T, Gutierrez-Gutierrez L, Sanchez-Hurtado LA, Martinez-Rodriguez N, Juarez-Cedillo E. Randomized controlled trial of multi-component cognitive stimulation therapy (SADEM) in community-dwelling demented adults. Journal of Alzheimer's Disease 2020;78:1033-45. [DOI: 10.3233/JAD-200574] - DOI - PubMed
Justo‐Henriques 2022 {published data only}
Kim 2016 {published data only}
Leroi 2019 {published and unpublished data}
Lin 2018 {published data only}
-
- Lin H-C, Yang Y-P, Cheng W-Y, Wang J-J. Distinctive effects between cognitive stimulation and reminiscence therapy on cognitive function and quality of life for different types of behavioural problems in dementia. Scandinavian Journal of Caring Sciences 2018;32(2):594-602. [DOI: 10.1111/scs.12484] - DOI - PubMed
Lok 2020 {published data only}
-
- Lok N, Buldukoglu K, Barcin E. Effects of the cognitive stimulation therapy based on Roy’s adaptation model on Alzheimer’s patients’ cognitive functions, coping-adaptation skills, and quality of life: a randomized controlled trial. Perspectives in Psychiatric Care 2020;56:581-92. [DOI: 10.1111/ppc.12472] - DOI - PubMed
Lopez 2020 {published data only}
Maci 2012 {published data only}
Mapelli 2013 {published data only}
Marinho 2021 {published and unpublished data}
-
- Marinho V, Bertrand E, Naylor R, Bomilcar I, Laks J, Spector A, et al. Cognitive stimulation therapy for people with dementia in Brazil (CST-Brasil): results from a single blind randomized controlled trial. International Journal of Geriatric Psychiatry 2021;36:286-93. [DOI: 10.1002/gps.5421] - DOI - PubMed
Middelstädt 2016 {published data only}
-
- Middelstaedt J, Folkerts A-K, Blawath S, Kalbe E. Cognitive stimulation for people with dementia in long-term care facilities: baseline cognitive level predicts cognitive gains, moderated by depression. Journal of Alzheimer's Disease 2016;54(1):253-68. [DOI: :10.3233/JAD-160181] - PubMed
Onder 2005 {published data only}
-
- Onder G, Zanetti O, Giacobini E, Frisoni GB, Bartorelli L, Carbone G, et al. Reality orientation therapy combined with cholinesterase inhibitors in Alzheimer's disease: randomised controlled trial. British Journal of Psychiatry 2005;187:450-5. - PubMed
Orgeta 2015 {published data only}
-
- Orgeta V, Leung P, Yates L, Kang S, Hoare Z, Henderson C, et al. Individual cognitive stimulation therapy for dementia: a clinical effectiveness and cost-effectiveness pragmatic, multicentre, randomised controlled trial. Health Technology Assessment 2015;19(64):7-73. [DOI: 10.3310/hta19640] - DOI - PMC - PubMed
-
- Orrell M, Yates L, Leung P, Kang S, Hoare Z, Whitaker C, et al. The impact of individual Cognitive Stimulation Therapy (iCST) on cognition, quality of life, caregiver health, and family relationships in dementia: a randomised controlled trial. PLOS Medicine 2017;14(3):e1002269. [DOI: 10.1371/journal.pmed.1002269] - DOI - PMC - PubMed
Orrell 2014 {published and unpublished data}
-
- Aguirre E, Spector A, Hoe J, Russell IT, Knapp M, Woods RT, et al. Maintenance Cognitive Stimulation Therapy (CST) for dementia: a single-blind, multi-centre, randomized controlled trial of maintenance CST vs. CST for dementia (study protocol). Trials 2010;11:46. [DOI: 10.1186/1745-6215-11-46] - DOI - PMC - PubMed
Paddick 2017 {published data only}
-
- Paddick S-M, Mkenda S, Mbowe G, Kisoli A, Gray WK, Dotchin CL, et al. Cognitive stimulation therapy as a sustainable intervention for dementia in sub-Saharan Africa: feasibility and clinical efficacy using a stepped-wedge design. International Psychogeriatrics 2017;29:979-89. [DOI: 10.1017/S1041610217000163] - DOI - PubMed
Rai 2021 {published data only}
Requena 2006 {published and unpublished data}
-
- Requena C, Lopez-Ibor MI, Maestu F, Campo P, Lopez-Ibor JJ, Ortiz T. Effects of cholinergic drugs and cognitive training on dementia. Dementia and Geriatric Cognitive Disorders 2004;18:50-4. - PubMed
-
- Requena C, Maestu F, Fernandez A, Ortiz T. Effects of cholinergic drugs and cognitive training on dementia: 2-year follow-up. Dementia and Geriatric Cognitive Disorders 2006;22:339-45. - PubMed
Spector 2001 {published data only}
-
- Spector A, Orrell M, Davies S, Woods B. Can reality orientation be rehabilitated? Development and piloting of an evidence-based programme of cognition-based therapies for people with dementia. Neuropsychological Rehabilitation 2001;11(3-4):377-97.
Spector 2003 {published data only}
-
- Knapp M, Thorgrimsen L, Patel A, Spector A, Hallam A, Woods B, et al. Cognitive stimulation therapy for people with dementia: cost-effectiveness analysis. British Journal of Psychiatry 2006;188:574-80. - PubMed
-
- Spector A, Thorgrimsen L, Woods B, Royan L, Davies S, Butterworth M, et al. Efficacy of an evidence-based cognitive stimulation therapy programme for people with dementia: randomised controlled trial. British Journal of Psychiatry 2003;183:248-54. - PubMed
Tanaka 2021 {published data only}
-
- Tanaka S, Yamagami T, Yamaguchi H. Effects of a group-based physical and cognitive intervention on social activity and quality of life for elderly people with dementia in a geriatric health service facility: a quasi-randomised controlled trial. Psychogeriatrics 2021;21:71-9. [DOI: 10.1111/psyg.12627] - DOI - PubMed
Tsantali 2017 {published data only}
-
- Tsantali E, Economidis D, Rigopoulou S. Testing the benefits of cognitive training vs. cognitive stimulation in mild Alzheimer's disease: a randomised controlled trial. Brain Impairment 2017;18(2):188-96. [DOI: ]
Young 2019 {published data only}
-
- Young DKW, Ng PYN, Kwok T, Ho F, Cheng D, Mak V, et al. The effects of an expanded cognitive stimulation therapy model on the improvement of cognitive ability of elderly with mild stage dementia living in a community - a randomized waitlist controlled trial. Aging & Mental Health 2019;23(7):855-62. [DOI: 10.1080/13607863.2018.1471586] - DOI - PubMed
References to studies excluded from this review
Alves 2014 {published data only}
-
- Alves J, Alves-Costa F, Magalhaes R, Goncalves OF, Sampaio A. Cognitive stimulation for Portuguese older adults with cognitive impairment: a randomized controlled trial of efficacy, comparative duration, feasibility, and experiential relevance. American Journal of Alzheimer's Disease and Other Dementias 2014;29:503-12. [DOI: 10.1177/1533317514522541] - DOI - PMC - PubMed
Apostolo 2013 {published data only}
-
- Apostolo J, Gil I, Rosa A, Almeida J, Fernandes A. The effect of cognitive stimulation on cognition in the elderly. Alzheimers & Dementia 2013;9(4 Suppl. 1):P650-1. [DOI: 10.1016/j.jalz.2013.05.1331 MISC1 - 20140418]
Apostolo 2014 {published data only}
Arcoverde 2008 {published data only}
-
- Arcoverde C, Deslandes A, Rangel A, Rangel A, Pavllo R, Nigri F, et al. Role of physical activity on the maintenance of cognition and activities of daily living in elderly with Alzheimer's disease. Arquivos de Neuro-Psiquiatria 2008;66(2b):323-7. - PubMed
Baglio 2015 {published data only}
Baines 1987 {published data only}
-
- Baines S, Saxby P, Ehlert K. Reality orientation and reminiscence therapy: a controlled cross-over study of elderly confused people. British Journal of Psychiatry 1987;151:222-31. - PubMed
Basak 2008 {published data only}
Brook 1975 {published data only}
-
- Brook P, Degun G, Mather M. Reality orientation, a therapy for psychogeriatric patient: a controlled study. British Journal of Psychiatry 1975;127:42-5. - PubMed
Buettner 2011 {published data only}
Calatayud 2022 {published data only}
-
- Calatayud E, Jimenez-Sanchez C, Calvo S, Brandin De la Cruz N, Herrero P, Gomez-Soria I. Effectiveness of cognitive stimulation personalized by the preexisting cognitive level in older adults: a randomized clinical trial. Topics in Geriatric Rehabilitation 2022;38:73-80. [DOI: 10.1097/TGR.0000000000000345] - DOI
Camargo 2015 {published data only}
Camargo 2019 {published data only}
-
- Camargo CHF, Ladeira MA, Serpa RA, Jobbins VA, Pucci CR, Welling LC, et al. The effectiveness of reality orientation therapy in the treatment of Parkinson disease dementia. American Journal of Alzheimer's Disease and Other Dementias 2019;34:124-30. [DOI: 10.1177/1533317518802461] - DOI - PMC - PubMed
Carlson 2008 {published data only}
-
- Carlson MC, Saczynski JS, Rebok GW, Seeman T, Glass TA, McGill S, et al. Exploring the effects of an "everyday" activity program on executive function and memory in older adults: Experience Corps. Gerontologist 2008;48(6):793-801. - PubMed
Cassinello 2008 {published data only}
-
- Cassinello DZ, Tarraga L, Fernandez-Ballesteros R. Cognitive plasticity in Alzheimer's disease patients receiving cognitive stimulation programmes. Psychology in Spain 2009;13(1):48-54.
-
- Cassinello DZ, Tarraga L, Fernandez-Ballesteros R. Cognitive plasticity in Alzheimer's disease patients receiving cognitive stimulation programs. Psicothema 2008;20:432-7. - PubMed
Cheng 2006 {published data only}
-
- Cheng ST, Chan ACM, Yu ECS. An exploratory study of the effect of Mahjong on the cognitive functioning of persons with dementia. International Journal of Geriatric Psychiatry 2006;21(7):611-7. - PubMed
Constantinidou 2008 {published data only}
-
- Constantinidou F, Thomas RD, Robinson L. Benefits of categorization training in patients with traumatic brain injury during post-acute rehabilitation: additional evidence from a randomized controlled trial. Journal of Head Trauma Rehabilitation 2008;23(5):312-28. - PubMed
Croisile 2006 {published data only}
-
- Croisile B. Memory stimulation. What rational? What exercises? Revue de Geriatrie 2006;31(6):421-33.
Davis 2001 {published data only}
-
- Davis RN, Massman PJ, Doody RS. Cognitive intervention in Alzheimer disease: a randomized placebo-controlled study. Alzheimer Disease and Associated Disorders 2001;15(1):1-9. - PubMed
Devita 2021 {published data only}
-
- Devita M, Masina F, Mapelli D, Anselmi P, Sergi G, Coin A. Acetylcholinesterase inhibitors and cognitive stimulation, combined and alone, in treating individuals with mild Alzheimer's disease. Aging: Clinical & Experimental Research 2021;33:3039-45. [DOI: 10.1007/s40520-021-01837-8] - DOI - PMC - PubMed
Eckroth‐Bucher 2009 {published data only}
Eggermont 2009a {published data only}
-
- Eggermont LH, Knol DL, Hol EM, Swaab DF, Scherder EJ. Hand motor activity, cognition, mood, and the rest-activity rhythm in dementia: a clustered RCT. Behavioural Brain Research 2009;196(2):271-8. - PubMed
Eggermont 2009b {published data only}
-
- Eggermont LH, Swaab DF, Hol EM, Scherder EJ. Walking the line: a randomised trial on the effects of a short term walking programme on cognition in dementia. Journal of Neurology, Neurosurgery and Psychiatry 2009;80(7):802-4. - PubMed
Evans 2009 {published data only}
-
- Evans JJ, Greenfield E, Wilson BA, Bateman A. Walking and talking therapy: improving cognitive-motor dual-tasking in neurological illness. Journal of the International Neuropsychological Society 2009;15(1):112-20. - PubMed
Faggian 2007 {published data only}
-
- Faggian S. An intervention protocol on cognitive abilities for subjects with severe cognitive impairment. Giornale di Gerontologia 2007;55(3):134-43.
Fanto 2002 {published data only}
-
- Fanto F, Tisci C, Molaschi M, Ostacoli L, Furlan PM, Riondato A, et al. Long-term reality orientation therapy for subjects with dementia in an Italian suburban setting. In: 8th International Conference on Alzheimer's Disease and Related Disorders; 2002 July 20-25, Stockholm, Sweden. 2002:Abstract No 1966.
Farina 2006a {published data only}
-
- Farina E, Mantovani F, Fioravanti R, Pignatti R, Chiavari L, Imbornone E, et al. Evaluating two group programmes of cognitive training in mild-to-moderate AD: is there any difference between a 'global' stimulation and a 'cognitive-specific' one? Aging & Mental Health 2006;10(3):211-8. - PubMed
Farina 2006b {published data only}
-
- Farina E, Mantovani F, Fioravanti R, Rotella G, Villanelli F, Imbornone E, et al. Efficacy of recreational and occupational activities associated to psychologic support in mild to moderate Alzheimer disease - a multicenter controlled study. Alzheimer Disease & Associated Disorders 2006;20(4):275-82. - PubMed
Fernandez‐Calvo 2010 {published data only}
-
- Fernandez-Calvo B, Contador I, Serna A, De Lucena VM, Ramos F. The effect of an individual or group intervention format in cognitive stimulation of patients with Alzheimer's disease [El efecto del formato de intervencion individual o grupal en la estimulacion cognitiva de pacientes con enfermedad de Alzheimer]. Revista de Psicopatología y Psicología Clínica 2010;15:115-23.
Ferrario 1991 {published data only}
-
- Ferrario E, Cappa G, Molaschi M, Rocco M, Fabris F. Reality orientation therapy in institutionalized elderly patients: preliminary results. Archives of Gerontology and Geriatrics 1991;12 Suppl 2:139-42.
Folkerts 2018 {published data only}
-
- Folkerts AK, Dorn ME, Roheger M, Maassen M, Koerts J, Tucha O, et al. Cognitive stimulation for individuals with Parkinson's disease dementia living in long-term care: preliminary data from a randomized crossover pilot study. Parkinson's Disease 2018;8104673:no pagination. [DOI: 10.1155/2018/8104673] - DOI - PMC - PubMed
Gerber 1991 {published data only}
-
- Gerber GJ, Prince PN, Snider HG, Atchison K, Dubois L, Kilgour JA. Group activity and cognitive improvement among patients with Alzheimer's disease. Hospital and Community Psychiatry 1991;42(8):843-5. - PubMed
Goldstein 1982 {published data only}
-
- Goldstein G. An evaluation of reality orientation therapy. Journal of Behavioral Assessment 1982;4(2):165-78.
Gonzalez‐Abraldes 2010 {published data only}
-
- Gonzalez-Abraldes I, Millan-Calenti JC, Balo-Garcia A, Tubio J, Lorenzo T, Maseda A. Accessibility and usability of computer-based cognitive stimulation: telecognitio. Revista Espanola de Geriatria y Gerontologia 2010;45(1):26-9. - PubMed
Green 2009 {published data only}
-
- Green HA, Patterson K. Jigsaws - a preserved ability in semantic dementia. Neuropsychologia 2009;47(2):569-76. - PubMed
Greenaway 2008 {published data only}
Han 2017 {published data only}
-
- Han JW, Lee H, Hong JW, Kim K, Kim T, Byun HJ, et al. Multimodal cognitive enhancement therapy for patients with mild cognitive impairment and mild dementia: a multi-center, randomized, controlled, double-blind, crossover trial. Journal of Alzheimer's Disease 2017;55:787-96. [DOI: 10.3233/JAD-160619] - DOI - PubMed
Hanley 1981 {published data only}
-
- Hanley IG, McGuire RJ, Boyd WD. Reality orientation and dementia: a controlled trial of two approaches. British Journal of Psychiatry 1981;138:10-4. - PubMed
Hill 2014 {published data only}
Holden 1978 {published data only}
-
- Holden UP, Sinebruchow A. Reality orientation therapy: a study investigating the value of this therapy in the rehabilitation of elderly people. Age and Ageing 1978;7(2):83-90. - PubMed
Johnson 1981 {published data only}
-
- Johnson CH, McLaren SM, McPherson FM. The comparative effectiveness of three versions of 'classroom' reality orientation. Age and Ageing 1981;10(1):33-5. - PubMed
Justo‐Henriques 2019 {published data only}
Kim 2015 {published data only}
-
- Kim KW, Han JW, Yoon JC, Ryu S-H, Lee N-J, Hong JW, et al. Effects of multimodal cognitive enhancement therapy (MCET) for people with mild cognitive impairment and early stage dementia: a randomized, controlled, double-blind, cross-over trial. Alzheimers & Dementia 2015;11(7 Suppl. 1):P465.
Kim 2020 {published data only}
Kolanowski 2016 {published data only}
-
- Kolanowski A, Fick D, Litaker M, Mulhall P, Clare L, Hill N, et al. Effect of cognitively stimulating activities on symptom management of delirium superimposed on dementia: a randomized controlled trial. Journal of American Geriatrics Society 2016;64:2424-32. [DOI: 10.1111/jgs.14511] - DOI - PMC - PubMed
Liu 2021 {published data only}
Luttenberger 2019 {published data only}
-
- Luttenberger K, Graessel E, Behrndt EM, Ozbe D, Donath C, Scheel J. Responder analysis of a multicomponent non-pharmacological intervention (MAKS) for people with cognitive impairment in the German day-care study (DeTaMAKS). Frontiers in Psychiatry 2019;10:587. [DOI: 10.3389/fpsyt.2019.00587] - DOI - PMC - PubMed
Matsuda 2007 {published data only}
-
- Matsuda O. Cognitive stimulation therapy for Alzheimer's disease: the effect of cognitive stimulation therapy on the progression of mild Alzheimer's disease in patients treated with donepezil. International Psychogeriatrics 2007;19(2):241-52. - PubMed
McCormick 2019 {published data only}
Menna 2016 {published data only}
Meza‐Kubo 2009 {published data only}
-
- Meza-Kubo V, Gonzalez-Fraga A, Moran AL, Tentori M. Augmenting cognitive stimulation activities in a nursing home through pervasive computing. In: La-Web: 2009 Latin American Web Congress. 2009:8-15.
Milev 2008 {published data only}
Mudge 2008 {published data only}
-
- Mudge AM, Giebel AJ, Cutler AJ. Exercising body and mind: an integrated approach to functional independence in hospitalized older people. Journal of the American Geriatrics Society 2008;56(4):630-5. - PubMed
Muniz 2015 {published data only}
Newson 2006 {published data only}
-
- Newson R, Kemps E. The influence of physical and cognitive activities on simple and complex cognitive tasks in older adults. Experimental Aging Research 2006;32(3):341-62. - PubMed
Niu 2010 {published data only}
Okamura 2018 {published data only}
Olazaran 2004 {published data only}
-
- Olazaran J, Muniz R, Reisberg B, Pena-Casanova J, Del Ser T, Cruz-Jentoft AJ, et al. Benefits of cognitive-motor intervention in MCI and mild to moderate Alzheimer disease. Neurology 2004;63:2348-53. - PubMed
Oliveira 2021 {published data only}
-
- Oliveira J, Gamito P, Souto T, Conde R, Ferreira M, Corotnean T, et al. Virtual reality-based cognitive stimulation on people with mild to moderate dementia due to Alzheimer's disease: a pilot randomized controlled trial. International Journal of Environmental Research & Public Health 2021;18:16. [DOI: 10.3390/ijerph18105290] - DOI - PMC - PubMed
Onieva‐Zafra 2018 {published data only}
-
- Onieva-Zafra MD, Hernandez-Garcia L, Gonzalez-del-Valle MT, Parra-Fernandez ML, Fernandez-Martinez E. Music intervention with Reminiscence Therapy and Reality Orientation for elderly people with Alzheimer disease living in a nursing home: a pilot study. Holistic Nursing Practice 2018;32:43-50. [DOI: 10.1097/HNP.0000000000000247] - DOI - PubMed
Orrell 2005 {published data only}
-
- Orrell M, Spector A, Thorgrimsen L, Woods B. A pilot study examining the effectiveness of Maintenance Cognitive Stimulation Therapy (MCST) for people with dementia. International Journal of Geriatric Psychiatry 2005;20:446-51. - PubMed
Perkins 2022 {published data only}
Piras 2017 {published data only}
Quayhagen 1995 {published data only}
-
- Corbeil RR, Quayhagen MP, Quayhagen M. Intervention effects on dementia caregiving interaction: a stress-adaptation modeling approach. Journal of Aging and Health 1999;11(1):79-95. - PubMed
-
- Quayhagen MP, Quayhagen M, Corbeil RR, Roth PA, Rodgers JA. A dyadic remediation program for care recipients with dementia. Nursing Research 1995;44(3):153-9. - PubMed
Quayhagen 2000 {published data only}
-
- Quayhagen MP, Quayhagen M, Corbeil RR, Hendrix RC, Jackson JE, Snyder L, et al. Coping with dementia: evaluation of four non pharmacologic interventions. International Psychogeriatrics 2000;12(2):249-65. - PubMed
Raggi 2007 {published data only}
Reeve 1985 {published data only}
-
- Reeve W, Ivison D. Use of environmental manipulation and classroom and modified informal reality orientation with institutionalized, confused elderly patients. Age and Ageing 1985;14(2):119-21. - PubMed
Riegler 1980 {published data only}
-
- Riegler J. Comparison of a reality orientation program for geriatric patients with and without music. Journal of Music Therapy 1980;17(1):26-33. - PubMed
Rueda 2021 {published data only}
Ruiz Sanchez de Leon 2007 {published data only}
-
- Ruiz Sanchez De Leon JM, Llanero Luque M. Computer-based cognitive training and donepezil: combined therapy effects in cognitive impairment. Mapfre Medicina 2007;18(1):25-33.
Schecker 2013 {published data only}
-
- Schecker M. Cognitive interventions in mild Alzheimer's disease. In: Europe Challenges the Burden of Mental Disorders. 21st European Congress of Psychiatry, European Psychiatric Association; 2013 April 6-9; Nice (France). 2013.
Schmitter‐Edgecombe 2008 {published data only}
Scott 2003 {published data only}
-
- Scott J, Clare L. Do people with dementia benefit from psychological interventions offered on a group basis? Clinical Psychology and Psychotherapy 2003;10(3):186-96.
Silva 2017 {published data only}
Silva 2021 {published data only}
Skov 2022 {published data only}
-
- Skov SS, Nielsen MBD, Krolner RF, Oksnebjerg L, Ronbol Lauridsen SM. A multicomponent psychosocial intervention among people with early-stage dementia involving physical exercise, cognitive stimulation therapy, psychoeducation and counselling: results from a mixed-methods study. Dementia 2022;21:316-34. [DOI: 10.1177/14713012211040683] - DOI - PubMed
Smith 2009 {published data only}
-
- Smith GE, Housen P, Yaffe K, Ruff R, Kennison RF, Mahncke HW, et al. A cognitive training program based on principles of brain plasticity: results from the improvement in memory with plasticity-based adaptive cognitive training (IMPACT) study. Journal of the American Geriatrics Society 2009;57(4):594-603. - PMC - PubMed
Tadaka 2004 {published data only}
-
- Tadaka E, Kanagawa K. A randomized controlled trial of a group care program for community-dwelling elderly people with dementia. Japan Journal of Nursing Science 2004;1:19-25.
Tanaka 2017 {published data only}
Tarraga 2006 {published data only}
-
- Tarraga L, Badenas S, Modinos G, Espinosa A, Diego S, Balcells J, et al. Randomized pilot study to evaluate the efficacy of an interactive multimedia internet-based tool for the cognitive stimulation of patients with Alzheimer's disease. In: 57th Annual Meeting of the American Academy of Neurology; 2005 April; Miami Beach. 2005:P01.138.
-
- Tarraga L, Boada M, Modinos G, Espinosa A, Diego S, Morera A, et al. Interactive cognitive stimulation with a computer and Alzheimer's disease. Neuroscientist 2007;13(2):97.
-
- Tarraga L. Randomised pilot study to evaluate the efficacy of an interactive multimedia system for the cognitive stimulation of Alzheimer's disease patients. In: 1st International Consensus Conference: Non pharmacological Therapies for Alzheimer's, 2005 May 12-13; Madrid. 2005:35-6.
Thickpenny‐Davis 2007 {published data only}
-
- Thickpenny-Davis KL, Barker-Collo SL. Evaluation of a structured group format memory rehabilitation program for adults following brain injury. Journal of Head Trauma Rehabilitation 2007;22:303-13. - PubMed
Tsai 2008 {published data only}
-
- Tsai AY, Yang M, Lan C, Chen C. Evaluation of effect of cognitive intervention programs for the community-dwelling elderly with subjective memory complaints. International Journal of Geriatric Psychiatry 2008;23(11):1172-4. - PubMed
Tsai 2019 {published data only}
-
- Tsai AY, Lee MC, Lai CC, Chou YC, Su CY. The outcomes of Cognitive Stimulation Therapy (CST) for community-dwelling older adults with cognitive decline in Taiwan. Topics in Geriatric Rehabilitation 2019;35:306-12. [DOI: 10.1097/TGR.0000000000000248] - DOI
Van Zon 2016 {published data only}
Wallis 1983 {published data only}
-
- Wallis GG, Baldwin M, Higginbotham P. Reality orientation therapy - a controlled trial. British Journal of Medical Psychology 1983;56(3):271-7. - PubMed
Wenisch 2007 {published data only}
-
- Wenisch E, Cantegreil-Kallen I, De Rotrou J, Garrigue P, Moulin F, Batouche F, et al. Cognitive stimulation intervention for elders with mild cognitive impairment compared with normal aged subjects: preliminary results. Aging Clinical & Experimental Research 2007;19(4):316-22. - PubMed
Wettstein 2004 {published data only}
-
- Wettstein A, Schmid R, Konig M. Who participates in psychosocial interventions for caregivers of patients with dementia? Dementia and Geriatric Cognitive Disorders 2004;18(1):80-6. - PubMed
Williams 1987 {published data only}
-
- Williams R, Reeve W, Ivison D, Kavanagh D. Use of environmental manipulation and modified informal reality orientation with institutionalized, confused elderly subjects: a replication. Age and Ageing 1987;16(5):315-8. - PubMed
Woods 1979 {published data only}
-
- Woods RT. Reality orientation and staff attention: a controlled study. British Journal of Psychiatry 1979;134:502-7. - PubMed
Yamanaka 2013 {published data only}
-
- Yamanaka K, Kawano Y, Noguchi D, Nakaaki S, Watanabe N, Amano, et al. Effects of cognitive stimulation therapy Japanese version (CST-J) for people with dementia: a single-blind, controlled clinical trial.. Aging & Mental Health 2013;17:579-86. [DOI: 10.1080/13607863.2013.795742] - DOI - PMC - PubMed
Young 2020 {published data only}
Zanetti 1995 {published data only}
-
- Zanetti O, Frisoni GB, De Leo D, Dello Bueno M, Bianchetti A, Trabucchi M. Reality orientation therapy in Alzheimer disease: useful or not? A controlled study. Alzheimer Disease and Associated Disorders 1995;9(3):132-8. - PubMed
Zepelin 1981 {published data only}
-
- Zepelin H, Wolfe CS, Kleinplatz F. Evaluation of a year long reality orientation program. Journal of Gerontology 1981;36(1):70-7. - PubMed
Zientz 2007 {published data only}
-
- Zientz J, Rackley A, Chapman SB, Hopper T, Mahendra N, Cleary S. Evidence-based practice recommendations: caregiver-administered active cognitive stimulation for individuals with Alzheimer's disease. Journal of Medical Speech-Language Pathology 2007;15(3):27-34.
References to ongoing studies
ChiCTR1800018600 {published data only}
-
- ChiCTR1800018600. Evaluation on the effect of maintenance cognitive stimulation therapy for dementia patients. www.chictr.org.cn/showprojen.aspx?proj=26814 (first received 29 September 2018).
NCT04550975 {published data only}
-
- NCT04550975. Advanced Cognitive Stimulation Therapy (ACST). clinicaltrials.gov/ct2/show/NCT04550975 (first received 16 September 2020).
NCT04828434 {published data only}
-
- NCT04828434. Virtual individual Cognitive Stimulation Therapy: a proof of concept study (V-iCST). clinicaltrials.gov/ct2/show/NCT04828434 (first received 2 April 2021).
Additional references
ADI 2022
-
- Alzheimer's Disease International. Dementia statistics. www.alzint.org/about/dementia-facts-figures/dementia-statistics/ (accessed 7 December 2022).
Aguirre 2011
-
- Aguirre E, Spector A, Streater A, Hoe J, Woods B, Orrell M. Making a Difference 2: An evidence-based group programme to offer maintenance Cognitive Stimulation Therapy (CST) to people with dementia. London: Hawker Publications, 2011.
Aguirre 2014
Alexopoulos 1988
-
- Alexopoulos GS, Abrams RC, Young RC, Shamoian CA. Cornell Scale for depression in dementia. Biological Psychiatry 2008;23:271-84. - PubMed
Alzheimer's Research UK 2022
-
- Alzheimer's Research UK. Dementia Statistics Hub. www.alzint.org/about/dementia-facts-figures/dementia-statistics/ (accessed 7 December 2022).
Alzheimer's Society 2022
-
- Alzheimer's Society. Left to Cope Alone: the unmet support needs after a dementia diagnosis. London: Alzheimer's Society, 2022. [https://www.alzheimers.org.uk/sites/default/files/2022-07/left-to-cope-a...]
Bahar‐Fuchs 2019
Burton 1982
-
- Burton M. Reality orientation for the elderly: a critique. Journal of Advanced Nursing 1982;7:427-33. - PubMed
Cafferata 2021
Chan 2020
Chen 2019
Cheung 2021
Clare 2004
-
- Clare L, Woods RT. Cognitive training and cognitive rehabilitation for people with early-stage Alzheimer's disease: a review. Neuropsychological Rehabilitation 2004;14:385-401.
Collins 2020
-
- Collins RN, Kishita N. Prevalence of depression and burden among informal care-givers of people with dementia: a meta-analysis. Ageing & Society 2020;40:2355-92. [DOI: 10.1017/S0144686X19000527] - DOI
Cummings 1997
Cunningham 2019
-
- Cunningham C, Macfarlane S, Brodaty H. Language paradigms when behaviour changes with dementia: # BanBPSD. International Journal of Geriatric Psychiatry 2019;34:1109-13. - PubMed
Deeks 2021
-
- Deeks JJ, Higgins JPT, Altman DG (editors), Cochrane Statistical Methods Group. Chapter 10: Analysing data and undertaking meta-analysis. In: Higgins J, Thomas J, Chandler J, Cumpston M, Li T, Page M, et al (editors). Cochrane Handbook for Systematic Reviews of Interventions, version 6.2, Cochrane 2021. Available from training.cochrane.org/handbook. [www.training.cochrane.org/handbook]
Dietch 1989
-
- Dietch JT, Hewett LJ, Jones S. Adverse effects of reality orientation. Journal of American Geriatrics Society 1989;37:974-6. - PubMed
Folstein 1975
-
- Folstein MF, Folstein SE, McHugh PR. 'Mini Mental State': a practical method for grading the cognitive state of patients for the clinician. Journal of Psychiatric Research 1975;12:189-98. - PubMed
Gallacher 2005
-
- Gallacher J, Bayer A, Ben-Shlomo Y. Commentary: Activity each day keeps dementia away — does social interaction really preserve cognitive function? International Journal of Epidemiology 2005;34:872-3. - PubMed
Gibbor 2020a
Greene 1982
-
- Greene JG, Smith R, Gardiner M, Timbury GC. Measuring behavioural disturbance of elderly demented patients in the community and its effects on relatives: a factor analytic study. Age & Ageing 1982;11:121-6. - PubMed
Group EuroQol 1990
-
- Group EuroQol. EuroQoL: a new facility for the measurement of health-related quality of life. Health Policy 1990;16:199-208. - PubMed
Guyatt 2011
-
- Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1. Introduction - GRADE evidence profiles and summary of findings tables. Journal of Clinical Epidemiology 2011;64(4):383-94. - PubMed
Hall 2013
-
- Hall L, Orrell M, Stott J, Spector A. Cognitive stimulation therapy (CST): neuropsychological mechanisms of change. International Psychogeriatrics 2013;25:479-89. - PubMed
Hamilton 1959
-
- Hamilton M. The assessment of anxiety states by rating. British Journal of Medical Psychology 1959;32:50-5. - PubMed
Higgins 2011
-
- Higgins JPT, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. (updated March 2011). The Cochrane Collaboration, 2011. Available from: training.cochrane.org/handbook/archive/v5.1.
Holden 1995
-
- Holden UP, Woods RT. Positive Approaches to Dementia Care. 3rd edition. Edinburgh: Churchill Livingstone, 1995.
Holden 2020
Howard 2011
Hughes 1982
-
- Hughes CP, Berg L, Danziger WL, Coben LA, Martin RL. A new clinical scale for the staging of dementia. British Journal of Psychiatry 1982;140:566-72. - PubMed
Hultsch 1999
-
- Hultsch DF, Hertzog C, Small BJ, Dixon RA. Use it or lose it: engaged lifestyle as a buffer of cognitive decline in aging? Psychology & Aging 1999;14(2):245-63. - PubMed
Huntley 2015
Kaddour 2020
Kim 2017
Kitwood 1997
-
- Kitwood T. Dementia Reconsidered: The Person Comes First. Buckingham: Open University Press, 1997.
Knapp 2022
-
- Knapp M, Bauer A, Wittenberg R, Comas-Herrera A, Cyhlarova E, Hu B, et al. What are the current and projected future cost and health-related quality of life implications of scaling up cognitive stimulation therapy? International Journal of Geriatric Psychiatry 2022;37:1-10. [DOI: 10.1002/gps.5633] - DOI - PubMed
Kudlicka 2019
Leung 2018
-
- Leung P. People's experiences of cognitive stimulation therapy: a qualitative understanding. In: Yates LA, Yates J, Orrell M, Spector A, Woods B, editors(s). Cognitive Stimulation Therapy for Dementia: History, Evolution and Internationalism. London: Routledge, 2018:131-51.
Liu 2018
-
- Liu BTY, Au ACL, Wong GHY. Neuropsychological aspects of cognitive stimulation therapy. In: Yates, LA, Yates J, Orrell M, Spector A, Woods B, editors(s). Cognitive Stimulation Therapy for Dementia: History, Evolution and Internationalism. London: Routledge, 2018:153-73.
Livingston 2020
Lobbia 2019
-
- Lobbia A, Carbone E, Faggian S, Gardini S, Piras F, Spector A, et al. The efficacy of cognitive stimulation therapy (CST) for people with mild-to-moderate dementia. European Psychologist 2019;24:257-77. [DOI: 10.1027/1016-9040/a000342] - DOI
Logsdon 2002
-
- Logsdon RG, Gibbons LE, McCurry SM, Teri L. Assessing quality of life in older adults with cognitive impairment. Psychosomatic Medicine 2002;64:510-9. - PubMed
Macera 1993
Mohs 2000
-
- Mohs R. Neuropsychological assessment of patients with Alzheimer's disease. In: Bloom FE, Kupfer DJ, editors(s). Psychopharmacology: 4th Generation of Progress. American College of Neuropsychopharmacology, 2000.
Moniz‐Cook 2008
-
- Moniz-Cook E, Vernooij-Dassen M, Woods R, Verhey F, Chattat R, De Vugt M, et al, INTERDEM group. A European consensus on outcome measures for psychosocial intervention research in dementia care. Aging & Mental Health 2008;12:14-29. - PubMed
NICE 2018
-
- NICE (National Institute of Health and Care Excellence). Dementia: Assessment, Management and Support for People Living with Dementia and Their Carers. NICE guideline [NG97]. London: National Institute of Health and Care Excellence, 2018. [https://www.nice.org.uk/guidance/ng97/evidence] - PubMed
NICE‐SCIE 2006
-
- NICE-SCIE. Dementia: Supporting People with Dementia and their Carers in Health and Social Care: Clinical Guideline 42. London: NICE-SCIE, 2006.
Novak 1989
-
- Novak M, Guest C. Application of a multidimensional caregiver burden inventory. Gerontologist 1989;29:798-803. - PubMed
Orfanos 2020
Pattie 1979
-
- Pattie A, Gilleard C. Clifton Assessment Procedures for the Elderly (CAPE). Sevenoaks: Hodder & Stoughton, 1979.
Powell‐Proctor 1982
-
- Powell-Proctor L, Miller E. Reality orientation: a critical appraisal. British Journal of Psychiatry 1982;140:457-63. - PubMed
Prince 2011
-
- Prince M, Bryce R, Ferri C. World Alzheimer Report 2011: the Benefits of Early Diagnosis and Intervention. London: Alzheimer's Disease International, 2011. [http://www.alz.co.uk/research/WorldAlzheimerReport2011.pdf]
Prince 2014
-
- Prince M, Knapp M, Guerchet M, McCrone P, Prina M, Comas-Herrera A, et al. Dementia UK; Update. London: Alzheimer's Society, 2014.
Rai 2020
Richardson 2019
-
- Richardson M, Garner P, Donegan S. Interpretation of subgroup analyses in systematic reviews: a tutorial. Clinical Epidemiology & Global Health 2019;7:192-8. [DOI: 10.1016/j.cegh.2018.05.005] - DOI
Rosen 1984
-
- Rosen WG, Mohs RC, Davis KL. A new rating scale for Alzheimer's disease. American Journal of Psychiatry 1984;141:1356-64. - PubMed
Sabat 1994
-
- Sabat SR. Excess disability and malignant social psychology: a case study of Alzheimer's disease. Journal of Community & Applied Social Psychology 1994;4:157-66.
Salthouse 2006
-
- Salthouse TA. Mental exercise and mental aging: evaluating the validity of the “use it or lose it” hypothesis. Perspectives on Psychological Science 2006;1:68-87. - PubMed
Schepers 2012
-
- Schepers AK, Orrell M, Shanahan N, Spector A. Sense of competence in Dementia Care Staff (SCIDS) scale: development, reliability, and validity. International Psychogeriatrics 2012;24:1153-62. [DOI: ] - PubMed
Schrag 2012
-
- Schrag A, Schott JM, Alzheimer's Disease Neuroimaging Initiative. What is the clinically relevant change on the ADAS-Cog? Journal of Neurology, Neurosurgery & Psychiatry 2012;83(2):171-3. - PubMed
Shankar 1999
-
- Shankar KK, Walker M, Frost D, Orrell MW. The development of a valid and reliable scale for rating anxiety in dementia (RAID). Aging & Mental Health 1999;3:39-49.
Small 2002
Smith 2008
-
- Smith BW, Dalen J, Wiggins K, Tooley E, Christopher P, Bernard J. The brief resilience scale: assessing the ability to bounce back. International Journal of Behavioral Medicine 2008;15:194-200. - PubMed
Spector 2000b
Spector 2006
-
- Spector A, Thorgrimsen L, Woods B, Orrell M. Making a Difference: an Evidence-Based Group Programme to Offer Cognitive Stimulation Therapy (CST) to People with Dementia. London: Hawker Publications, 2006.
Spector 2010
-
- Spector A, Orrell M, Woods B. Cognitive Stimulation Therapy (CST): effects on different areas of cognitive function for people with dementia. International Journal of Geriatric Psychiatry 2010;25:1253-8. - PubMed
Spector 2011
-
- Spector A, Gardner C, Orrell M. The impact of Cognitive Stimulation Therapy groups on people with dementia: views from participants, their carers and group facilitators. Aging & Mental Health 2011;15(8):945-9. - PubMed
Spector 2020
-
- Spector A, Woods B, Stoner CR, Orrell M. Making a Difference - 1. 2nd revised edition. London: Hawker Publications, 2020. [ISBN: 9781874790891]
Spruytte 2002
-
- Spruytte N, Van Audenhove C, Lammertyn F, Storms G. The quality of the caregiving relationship in informal care for older adults with dementia and chronic psychiatric patients. Psychology and Psychotherapy: Theory, Research and Practice 2002;75(3):295-311. - PubMed
Streater 2020
-
- Streater A, Yates L, Orrell M, Rosen J, Taylor Smith A, Schneider J. Interacting with television in one’s own home: the development of a cognitive stimulation television pilot episode for older people with dementia (Innovative Practice). Dementia 2020;19(8):2881-8. [DOI: 10.1177/1471301219836001] - DOI - PubMed
Tarlov 1989
-
- Tarlov AR, Ware JE, Greenfield S. The Medical Outcomes Study: an application of methods for monitoring the results of medical care. Journal of the American Medical Association 1989;262:925-30. - PubMed
Taulbee 1966
-
- Taulbee LR, Folsom JC. Reality orientation for geriatric patients. Hospital & Community Psychiatry 1966;17:133-5. - PubMed
Terada 2015
-
- Terada S, Oshima E, Ikeda C, Hayashi S, Yokota O, Uchitomi Y. Development and evaluation of a short version of the quality of life questionnaire for dementia. International Psychogeriatrics 2015;27:103-10. - PubMed
Wagnild 2009
-
- Wagnild GM. The Resilience Scale: User's Guide for the US English Version of the Resilience Scale and the 14-Item Resilience Scale (RS-14). Worden, MT: Resilience Center, 2009.
Wan 2014
Ware 1996
-
- Ware JE Jr, Kosinski M, Keller SD. A 12 item short form health survey: construction of scales and preliminary tests of reliability and validity. Medical Care 1996;34:220-3. - PubMed
Watt 2021
Webster 2017
-
- Webster L, Groskreutz D, Grinbergs-Saull A, Howard R, O'Brien JT, Mountain G, et al. Core outcome measures for interventions to prevent or slow the progress of dementia for people living with mild to moderate dementia: systematic review and consensus recommendations. PLOS One 2017;12(6):e0179521. [DOI: 10.1371/journal.pone.0179521] - DOI - PMC - PubMed
Wolverson 2019
-
- Wolverson E, Birtles H, Moniz-Cook E, James I, Brooker D, Duffy F. Naming and framing the behavioural and psychological symptoms of dementia (BPSD) paradigm: professional stakeholder perspectives. OBM Geriatrics 2019;3:1-19. [DOI: 10.21926/obm.geriatr.1904080] - DOI
Wolverson 2021
Woods 1977
-
- Woods RT, Britton PG. Psychological approaches to the treatment of the elderly. Age & Ageing 1977;6:104-12. - PubMed
Woods 2002
-
- Woods B. Editorial: Reality Orientation: a welcome return? Age & Ageing 2002;31:155-6. - PubMed
Woods 2006
-
- Woods B, Thorgrimsen L, Spector A, Royan L, Orrell M. Improved quality of life and cognitive stimulation therapy in dementia. Aging & Mental Health 2006;10(3):219-26. - PubMed
Woods 2014
-
- Woods B, Russell I. Randomisation and Chance-Based Designs in Social Care Research. NIHR School for Social Care Research Methods Review 17. London: NIHR SSCR, 2014. [http://sscr.nihr.ac.uk/PDF/MR/MR17.pdf]
Woods 2016
-
- Woods RT, Orrell M, Bruce E, Edwards RT, Hoare Z, Hounsome B, et al. REMCARE: Pragmatic multi-centre randomised trial of reminiscence groups for people with dementia and their family carers: effectiveness and economic analysis. PLOS One 2016;11:e0152843. [DOI: 10.1371/journal.pone.0152843] - DOI - PMC - PubMed
Woods 2018a
-
- Woods B. CST: development process. In: Yates L, Yates J, Orrell M, Spector A, Woods B, editors(s). Cognitive Stimulation Therapy for Dementia: History, Evolution and Internationalism. Abingdon: Routledge, 2018:33-47.
Woods 2018b
Yates 2014
-
- Yates L, Orrell M, Leung P, Spector A, Woods B, Orgeta V. Making a Difference 3. Individual Cognitive Stimulation Therapy: a Manual for Carers. London: Hawker, 2014.
Yesavage 1983
-
- Yesavage JA, Brink TL, Rose TL. Development and validation of a geriatric depression scale: a preliminary report. Journal of Psychiatric Research 1983;17:37-49. - PubMed
Zarit 1980
-
- Zarit SH, Reever KE, Bach-Peterson J. Relatives of the impaired elderly: correlates of feelings of burden. Gerontologist 1980;20:649-55. - PubMed
Zigmond 1983
-
- Zigmond AS, Snaith RP. The Hospital Anxiety and Depression scale. Acta Psychiatrica Scandinavica 1983;67:361-70. - PubMed
References to other published versions of this review
Aguirre 2013
Spector 2000a
-
- Spector A, Davies S, Woods B, Orrell M. Reality orientation for dementia: a systematic review of the evidence for its effectiveness. Gerontologist 2000;40(2):206-12. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous