

Use of Maternal-Fetal Medicine Subspecialist Services by Commercially Insured Pregnant People
- PMID: 39804642
- PMCID: PMC11731212
- DOI: 10.1001/jamanetworkopen.2024.54565
Use of Maternal-Fetal Medicine Subspecialist Services by Commercially Insured Pregnant People
Abstract
Importance: Improving access to high-quality maternity care and reducing maternal morbidity and mortality are major policy priorities in the US. Previous research has primarily focused on access to general obstetric care rather than access to high-risk pregnancy care provided by maternal-fetal medicine subspecialists (MFMs).
Objective: To measure access to MFM services and determine patient factors associated with MFM service use, including MFM telemedicine.
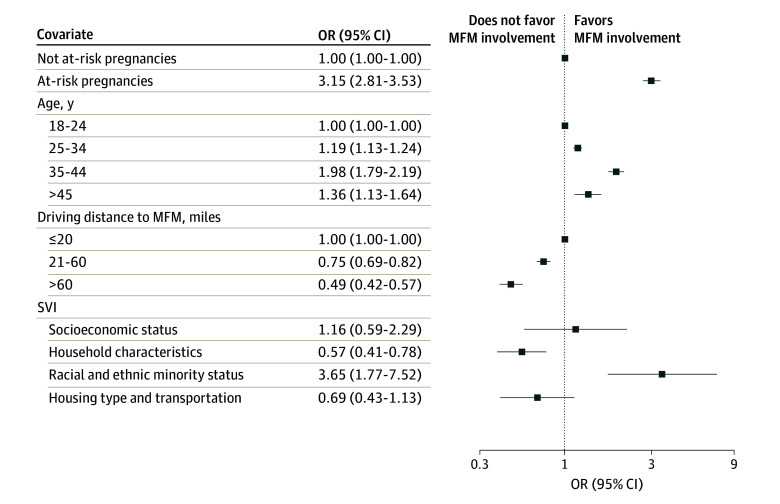
Design, setting, and participants: This cohort study identified pregnancies in commercial health insurance claims from the Health Care Cost Institute from 2016 to 2021. More than 2.1 million pregnancies were included, where age at delivery was 18 years or greater and people were continuously enrolled for the duration of their pregnancy. The association of patient and pregnancy covariates with MFM involvement in care was analyzed using logistic regression; and rates of telemedicine for pregnancies in urban and rural areas were reported over time. Data were analyzed from June 2022 to March 2024.
Main outcomes and measures: Primary study outcomes included whether a pregnancy ever had a service from an MFM, the type of MFM services provided, and whether MFM care occurred via telemedicine.
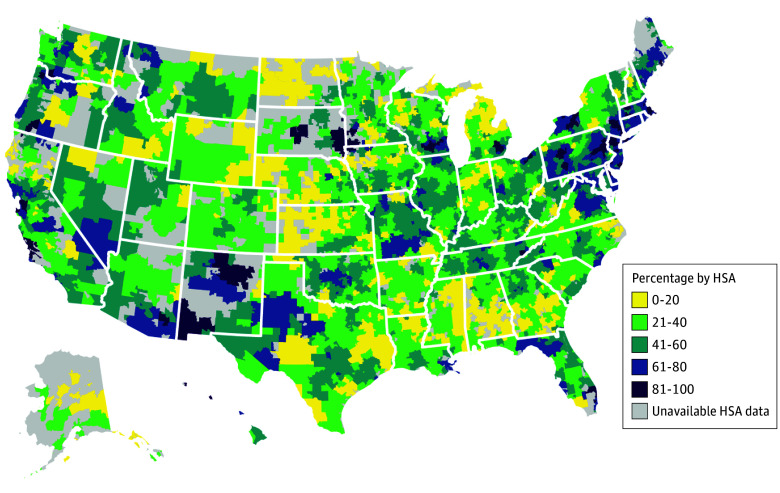
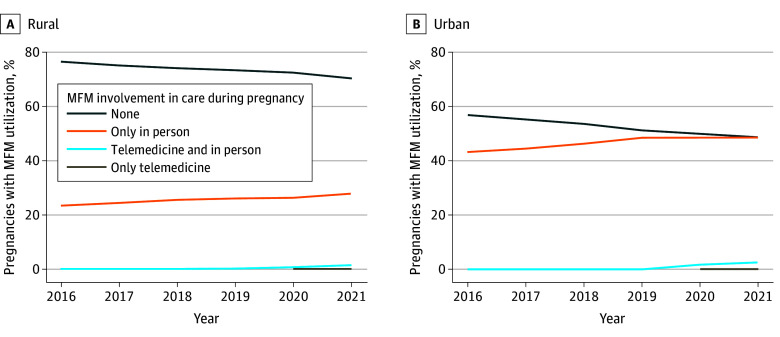
Results: There were 2 169 026 pregnancies among 1 968 091 unique people (1 325 212 [61.2%] aged 25 to 34 years). Among 1 625 237 pregnancies at risk for conditions that might require MFM involvement, 838 493 (51.6%) had an MFM service. Rates of MFM involvement in care varied considerably by geography, with pregnancies in rural areas having lower use than urban areas. Use of telemedicine-enabled MFM care increased in 2020 and 2021 but remained low: in 2021, 2.7% of urban pregnancies (7535 of 276 599) and 1.7% of rural pregnancies (550 of 32 949) received telemedicine-enabled MFM care.
Conclusions and relevance: In this cohort study, access to MFM services varied across geography, even among pregnancies at risk for conditions that might require MFM involvement. These results suggested a need to improve access to MFM care for at-risk pregnancies and to further explore expanded access via telemedicine.
Conflict of interest statement
Figures
References
-
- Brigance C, Lucas R, Jones E, et al. . Nowhere to go: maternity care deserts across the U.S. (report No. 3). March of Dimes . 2022. Accessed December 2, 2024. https://www.marchofdimes.org/sites/default/files/2022-10/2022_Maternity_...
-
- World Health Organization . Trends in maternal mortality 2000 to 2017: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. 2019. Accessed October 18, 2023. https://iris.who.int/handle/10665/327595
-
- CMS . HHS to improve maternal health outcomes with new CMS care model that expands access to services, other proven maternal health approaches. Accessed February 13, 2024. https://www.cms.gov/newsroom/press-releases/hhs-improve-maternal-health-...
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
