

Can Contrast Injections Cause or Propagate Coronary Injuries? Insights From Vessel and Guiding Catheter Hemodynamics
- PMID: 39807240
- PMCID: PMC11725123
- DOI: 10.1016/j.jscai.2024.102396
Can Contrast Injections Cause or Propagate Coronary Injuries? Insights From Vessel and Guiding Catheter Hemodynamics
Abstract
Background: The mechanistic association between the hydraulic forces generated during contrast injection and the risk of coronary injury is poorly understood. In this study, we sought to evaluate whether contrast injections increase intracoronary pressures beyond resting levels and estimate the risk of hydraulic propagation of coronary dissections.
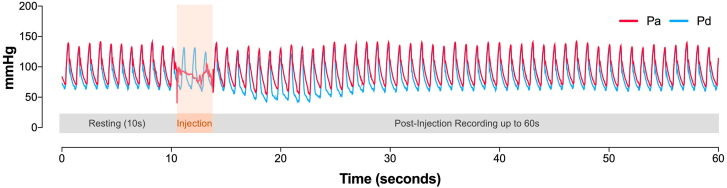
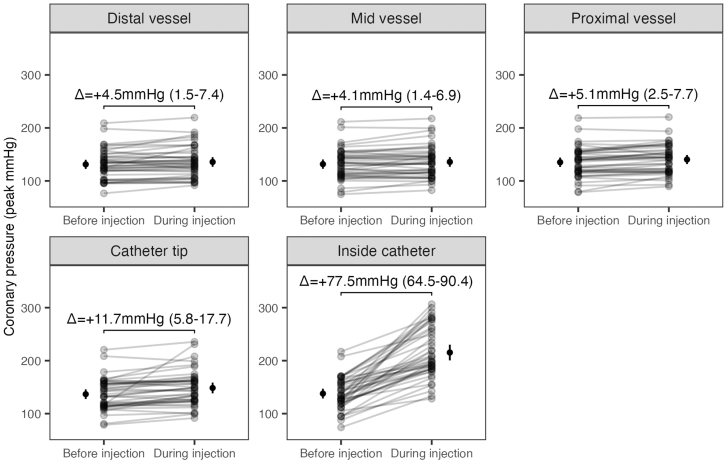
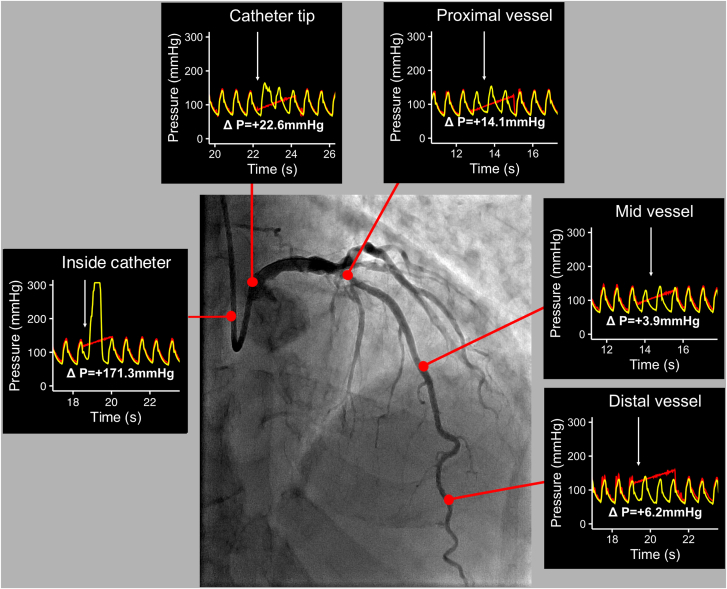
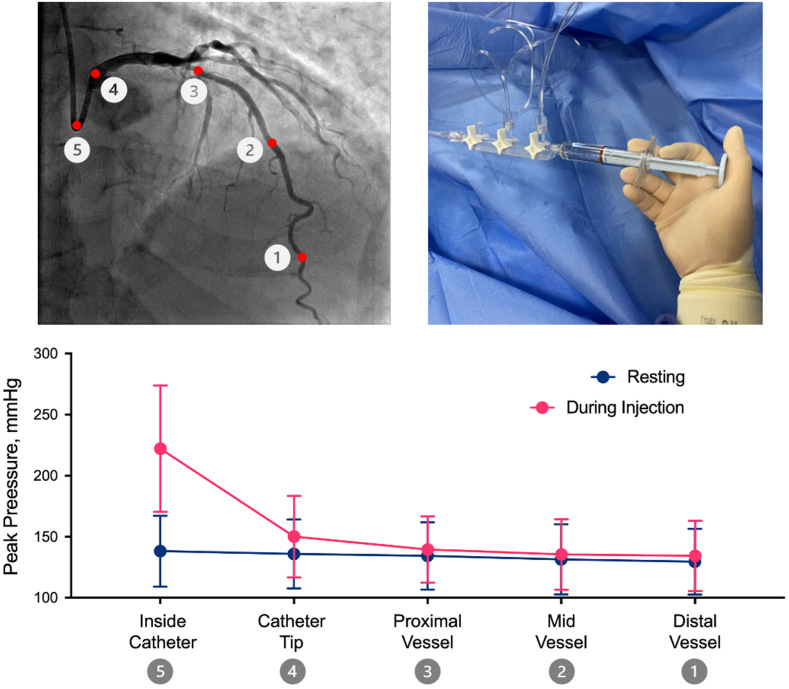
Methods: This is a prospective, single-arm, multicenter study that included patients with nonculprit, non-flow-limiting coronaries. A continuous 60-second pressure recording was taken at 5 predetermined locations during contrast injections: distal, mid, and proximal vessel, catheter tip, and inside the catheter. The primary end point was the change in intracoronary peak pressure between resting and injections in each location.
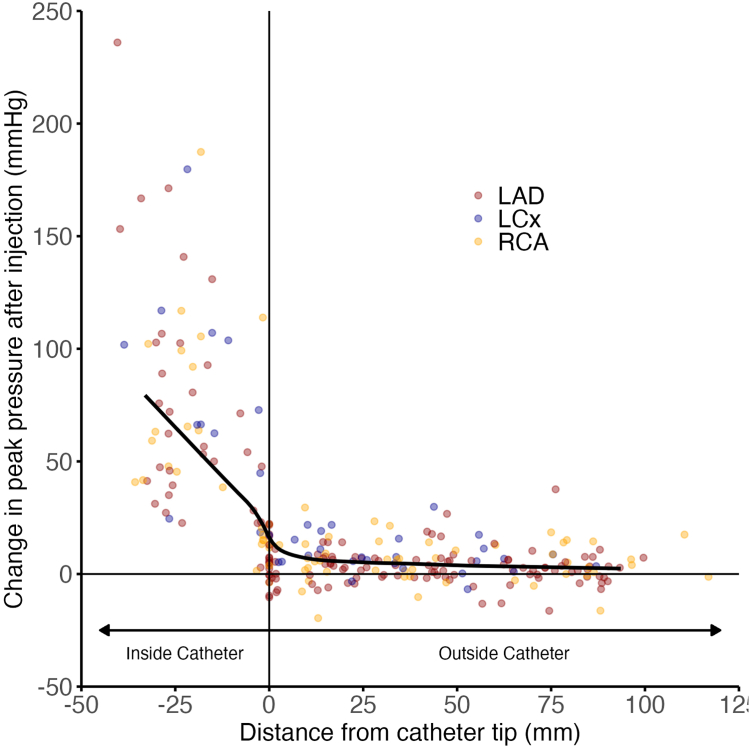
Results: A total of 269 pressure recordings (58 vessels; 52 patients) were analyzed. Injections led to a small increase in peak pressure in the distal (mean difference, +4.5 mm Hg; 95% CI, 1.5-7.4), mid (mean difference, +4.1 mm Hg; 95% CI, 1.4-6.9), and proximal (mean difference, +5.1 mm Hg; 95% CI, 2.5-7.7) vessel locations, and much higher increases at the catheter tip (mean difference, +11.7 mm Hg; 95% CI, 5.8-17.7) and inside the catheter (mean difference, +77.5 mm Hg; 95% CI, 64.5-90.4). Compared to the distal vessel, pressure changes were only significant at the catheter tip (+10 mm Hg; P < .01) and inside the catheter (+79.1 mm Hg; P < .01).
Conclusions: Contrast injections lead to negligible changes in intracoronary pressures beyond the catheter tip. Although it is sensible to minimize injections when coronary dissections are close to the catheter, it is unlikely that they would cause injuries beyond the catheter tip.
Keywords: chronic total occlusions; contrast; coronary angiography; coronary dissections; optical coherence tomography.
© 2024 The Author(s).
Figures


References
-
- Hiraide T., Sawano M., Shiraishi Y., et al. Impact of catheter-induced iatrogenic coronary artery dissection with or without postprocedural flow impairment: a report from a Japanese multicenter percutaneous coronary intervention registry. PLOS ONE. 2018;13(9) doi: 10.1371/journal.pone.0204333. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
