

Fracture liaison service (FLS) is associated with lower subsequent fragility fracture risk and mortality: NoFRACT (the Norwegian capture the fracture initiative)
- PMID: 39808195
- PMCID: PMC11882684
- DOI: 10.1007/s00198-024-07376-y
Fracture liaison service (FLS) is associated with lower subsequent fragility fracture risk and mortality: NoFRACT (the Norwegian capture the fracture initiative)
Abstract
Subsequent fracture rates and associated mortality were compared before and after the introduction of fracture liaison service (FLS). In 100,198 women and men, FLS was associated with 13% and 10% lower risk of subsequent fragility fractures and 18% and 15% lower mortality. The study suggests that FLS may prevent fractures.
Purpose: Efficient fracture prevention strategies are warranted to control the global fracture burden. We investigated the effect of a standardized fracture liaison service (FLS) intervention on subsequent fracture risk and mortality.
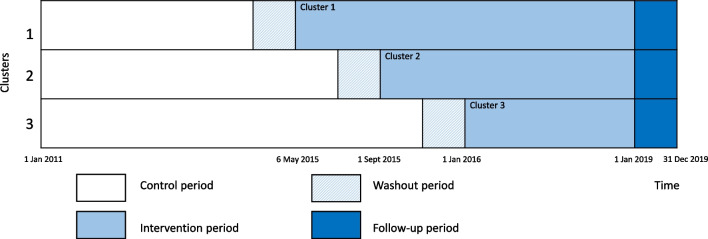
Methods: The NoFRACT study was designed as a multicenter, pragmatic, register-supported, stepped-wedge cluster-randomized trial. The FLS intervention was introduced in three clusters with 4-month intervals starting May 2015 through December 2018 and included evaluation of osteoporosis and treatment in patients over 50 years with a low-energy fracture. Based on data from the Norwegian Patient Registry, patients with index fractures were assigned to the control period (2011-2015) or intervention period (2015-2018) depending on the time of fracture. Rates of subsequent fragility fractures (distal forearm, proximal humerus, or hip) and all-cause mortality were calculated.
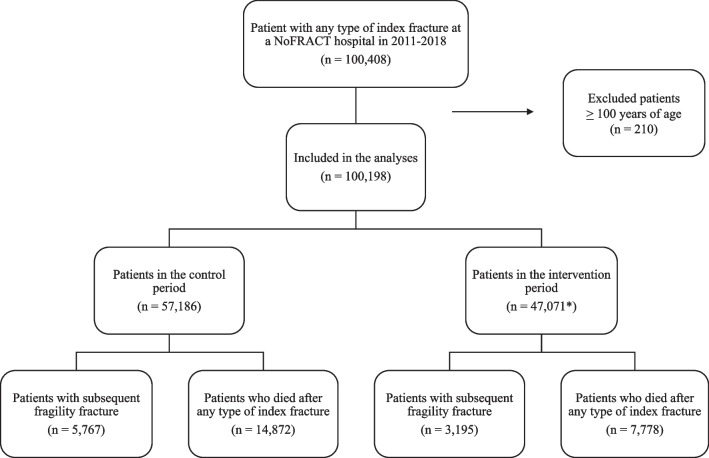
Results: A total of 100,198 patients (mean age 69.6 years) suffered an index fracture of any type. During a maximum follow-up of 4.7 years, 11% (6948) of the women and 6% (2014) of the men experienced a subsequent fragility fracture, and 20% (14,324) of the women and 22% (8,326) of the men died. FLS was associated with 13% lower subsequent fragility fracture risk in women (hazard ratio (HR) 0.87, 95% confidence intervals (CI) 0.83-0.92) and 10% in men (HR 0.90, 95% CI 0.81-0.99) and 18% lower mortality in women (HR 0.82, 95% CI 0.79-0.86) and 15% in men (HR 0.85, 95% CI 0.81-0.89).
Conclusion: A standardized FLS intervention was associated with a lower risk of subsequent fragility fractures and mortality and may contribute to reduce the global fracture burden.
Keywords: fracture liaison service; fragility fractures; osteoporosis; post-fracture mortality; secondary fracture prevention; stepped-wedge cluster-randomized trial.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: All procedures performed in the study were in accordance with the 1964 Helsinki Declaration and its later amendments. The study was approved by the Regional Committee of Medical and Health Research Ethics (REK 2015/334). The merging of data using the personal identification number and exemption from obtaining consent for the collection of data was approved by the Regional Committee of Medical and Health Research Ethics (REK 2015/334). A Data Protection Impact Assessment (DPIA) in agreement with the General Data Protection Regulation was performed by The University of Oslo. The study was approved by the Patient Data Protection Officer (PVO) at each of the hospitals and the PVO provided exemption from obtaining consent from the participants and authorized a secure research server for storage of the audit data. Conflict of interest: CA, CD, TB, TW, GH, JMS, IL, AKH, FIN, LN, TKO, and ÅB no support from any organization for the submitted work; FF reports lecturing fees from UCB and Amgen; TTB reports speaker fees from UCB, Amgen, Roche Diagnostics, and Pharma Prim and participation in an advisory board for UCB. Further, FF is president of the Fragility Fracture Network which is sponsored by Amgen, UCB, and Danone; JEG reports lecture fees from Ortomedic Norway, Smith and Nephew, Heraeus Medical, and LINK Norway; WF reports lecture fees from Ortomedic Norway and Zimmer Biomet Norway; EMA reports participation in the advisory board for UCB and Amgen; RMJ reports consulting fees from Norwegian Directorate of Health, Norwegian Diabetes Association, and Northern Norway Regional Health Authority and lecture fees from Novo Nordisk, Eli-Lilly, Astra-Zeneca, and Sanofi; US reports speaker and consulting fees from Amgen, UCB, and Novartis; EFE reports consultant fees from Novartis, UCB, Amgen, Takeda, and Pharma Medico and research support from Takeda and Amgen. Further, EFE has worked as a medical consultant for the Norwegian Osteoporosis Society; LBS reports speaker fees from Eli Lilly, Amgen, and UCB. Further, LBS is the president of Fragility Fracture Network Norway.
Figures
References
-
- Sambrook P, Cooper C (2006) Osteoporosis. Lancet 367(9527):2010–2018 - PubMed
-
- Svedbom A, Borgstöm F, Hernlund E, Ström O, Alekna V, Bianchi ML et al (2018) Quality of life for up to 18 months after low-energy hip, vertebral, and distal forearm fractures-results from the ICUROS. Osteoporos Int 29(3):557–566 - PubMed
-
- Alarkawi D, Bliuc D, Tran T, Ahmed LA, Emaus N, Bjornerem A et al (2020) Impact of osteoporotic fracture type and subsequent fracture on mortality: the Tromso Study. Osteoporos Int 31(1):119–130 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
