

Comparative application of MAFLD and MASLD diagnostic criteria on NAFLD patients: insights from a single-center cohort
- PMID: 39808219
- PMCID: PMC11732950
- DOI: 10.1007/s10238-024-01553-3
Comparative application of MAFLD and MASLD diagnostic criteria on NAFLD patients: insights from a single-center cohort
Abstract
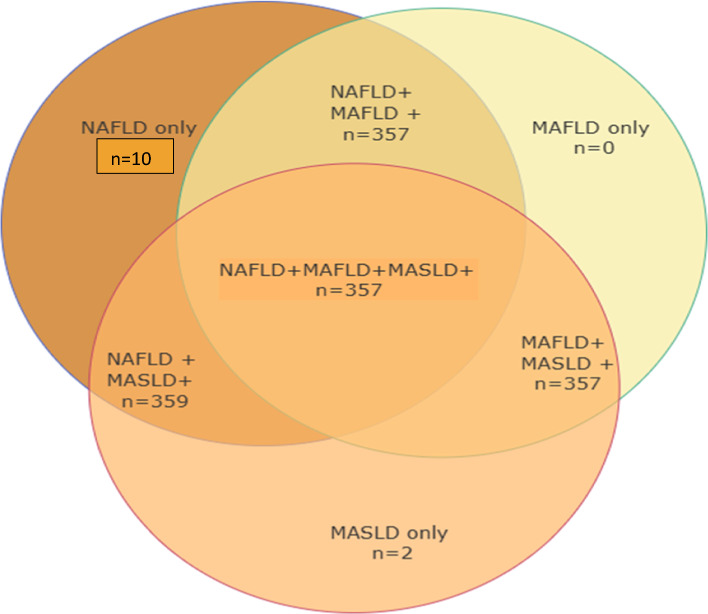
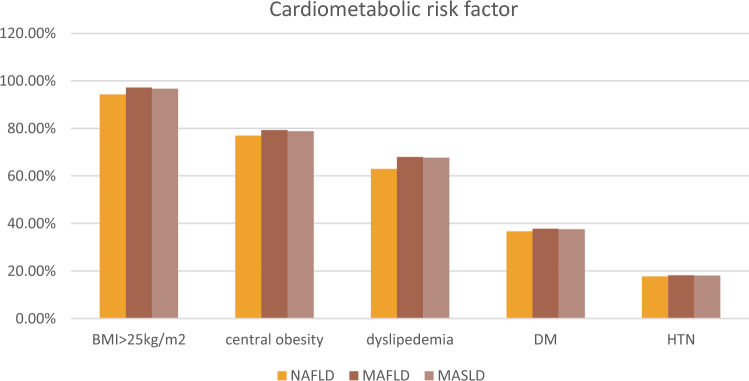
The diagnostic criteria for Metabolic Dysfunction-Associated Fatty Liver Disease (MAFLD) and Metabolic Associated Steatotic Liver Disease (MASLD) aim to refine the classification of fatty liver diseases previously grouped under Non-Alcoholic Fatty Liver Disease (NAFLD). This study evaluates the applicability of the MAFLD and MASLD frameworks in NAFLD patients, exploring their clinical utility in identifying high-risk patients. A total of 369 NAFLD patients were assessed using MAFLD and MASLD diagnostic criteria. Baseline characteristics, metabolic profiles, hepatic fibrosis, and cardiovascular risks were compared across the groups. Among NAFLD patients, 97.55% (n = 359) met MASLD criteria, and 97.01% (n = 357) fulfilled MAFLD criteria. Both frameworks MAFLD and MASLD captured overlapping populations, with MASLD encompassing slightly more cases. No significant differences were observed in metabolic risk factors, fibrosis indices (APRI, FIB-4, NAFLD fibrosis score), or cardiovascular risk (10-year ASCVD score). A small subset of lean NAFLD patients (10 cases) with distinct profiles remained uncategorized by either framework. Pure NAFLD cases (n = 10) were with mild insulin resistance (HOMA-IR: 3.07 ± 0.33) and slightly elevated LDL (102.5 ± 42.87 mg/dL), while fibrosis indices indicated low fibrosis risk. Steatosis indices supported the diagnosis of early-stage NAFLD with preserved liver function. These patients do not meet the criteria for inclusion in the MAFLD or MASLD frameworks, highlighting a gap in the current diagnostic systems. MAFLD and MASLD criteria align closely with NAFLD in capturing patients with metabolic risk with MASLD-enhanced inclusivity. Further refinement is required to address heterogeneity, particularly in lean NAFLD patients. Hypertension prevalence was comparable (17.4% in NAFLD, 18.2% in MAFLD, 17.8% in MASLD; p = 0.960), as was diabetes mellitus (36.7%, 37.8%, and 37.6%, respectively; p = 0.945). Body mass index was also similar across groups, with medians of 33.25, 33.6, and 33.4 kg/m2 (p = 0.731). Non-invasive markers of hepatic fibrosis, including APRI, FIB-4, and NAFLD fibrosis scores, did not differ significantly, with median FIB-4 scores around 1.05 (p = 0.953). Similarly, were the results of hepatic steatosis index and ASCVD score.
Keywords: Cardiovascular risk; Fibrosis; Hepatic steatosis; MAFLD; MASLD; NAFLD.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of Interest: The authors declare no competing interests. Ethics approval: “This study was conducted per the principles of the Declaration of Helsinki. This study was approved by the Ethics Committee of the National Liver Institute, Menoufia University as unique research and not a part of an approved student thesis. Informed consent was obtained from all patients or their legal representatives before enrolment in the study. Consent to participate and publish.: Not applicable.
Figures
Similar articles
-
Characterizing Nonalcoholic Fatty Liver Disease (NAFLD) in Lean Individuals at a Tertiary Care Hospital: A Cross-sectional Study.Euroasian J Hepatogastroenterol. 2024 Jul-Dec;14(2):198-204. doi: 10.5005/jp-journals-10018-1452. Epub 2024 Dec 27. Euroasian J Hepatogastroenterol. 2024. PMID: 39802861 Free PMC article.
-
Impact of nomenclature as metabolic associated steatotic liver disease on steatotic liver disease prevalence and screening: a prospective population survey in Asians.J Gastroenterol Hepatol. 2024 Aug;39(8):1636-1647. doi: 10.1111/jgh.16554. Epub 2024 May 2. J Gastroenterol Hepatol. 2024. PMID: 38695344
-
Metabolic dysfunction-associated fatty liver disease indicates more hepatic fibrosis than nonalcoholic fatty liver disease.Medicine (Baltimore). 2025 Feb 7;104(6):e41455. doi: 10.1097/MD.0000000000041455. Medicine (Baltimore). 2025. PMID: 39928810 Free PMC article.
-
Non-invasive Scores and Serum Biomarkers for Fatty Liver in the Era of Metabolic Dysfunction-associated Steatotic Liver Disease (MASLD): A Comprehensive Review From NAFLD to MAFLD and MASLD.Curr Obes Rep. 2024 Sep;13(3):510-531. doi: 10.1007/s13679-024-00574-z. Epub 2024 May 29. Curr Obes Rep. 2024. PMID: 38809396 Free PMC article. Review.
-
Why MASLD Lags Behind MAFLD: A Critical Analysis of Diagnostic Criteria Evolution in Metabolic Dysfunction-Associated Liver Diseases.Med Sci Monit. 2024 Jul 30;30:e945198. doi: 10.12659/MSM.945198. Med Sci Monit. 2024. PMID: 39075772 Free PMC article. Review.
Cited by
-
Triglyceride-glucose-waist circumference index: A powerful tool for metabolic dysfunction-associated steatotic liver disease.World J Hepatol. 2025 Jul 27;17(7):107668. doi: 10.4254/wjh.v17.i7.107668. World J Hepatol. 2025. PMID: 40747214 Free PMC article. Review.
-
MASLD: Prevalence, Mechanisms, and Sex-Based Therapies in Postmenopausal Women.Biomedicines. 2025 Apr 2;13(4):855. doi: 10.3390/biomedicines13040855. Biomedicines. 2025. PMID: 40299427 Free PMC article. Review.
References
-
- Mary ER, Jeffrey VL, Ratziu V, Sven MF, Arun JS, Kanwal F, Philip NN. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Annals Hepatol. 2024;29(1):1–15. - PubMed
-
- Portincasa P, Baffy G. Metabolic dysfunction-associated steatotic liver disease: evolution of the final terminology. Eur J Intern Med. 2024;124:35–9. 10.1016/j.ejim.2024.04.013. (Epub 2024 Apr 22 PMID: 38653634). - PubMed
-
- Eslam M, Sanyal AJ, George J, Sanyal A, Neuschwander-Tetri B, Tiribelli C, Younossi Z. MAFLD: a consensus-driven proposed nomenclature for metabolic associated fatty liver disease. Gastroenterology. 2020;158(7):1999–2014. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
