

Highly multiplexed imaging reveals prognostic immune and stromal spatial biomarkers in breast cancer
- PMID: 39808504
- PMCID: PMC11948582
- DOI: 10.1172/jci.insight.176749
Highly multiplexed imaging reveals prognostic immune and stromal spatial biomarkers in breast cancer
Abstract
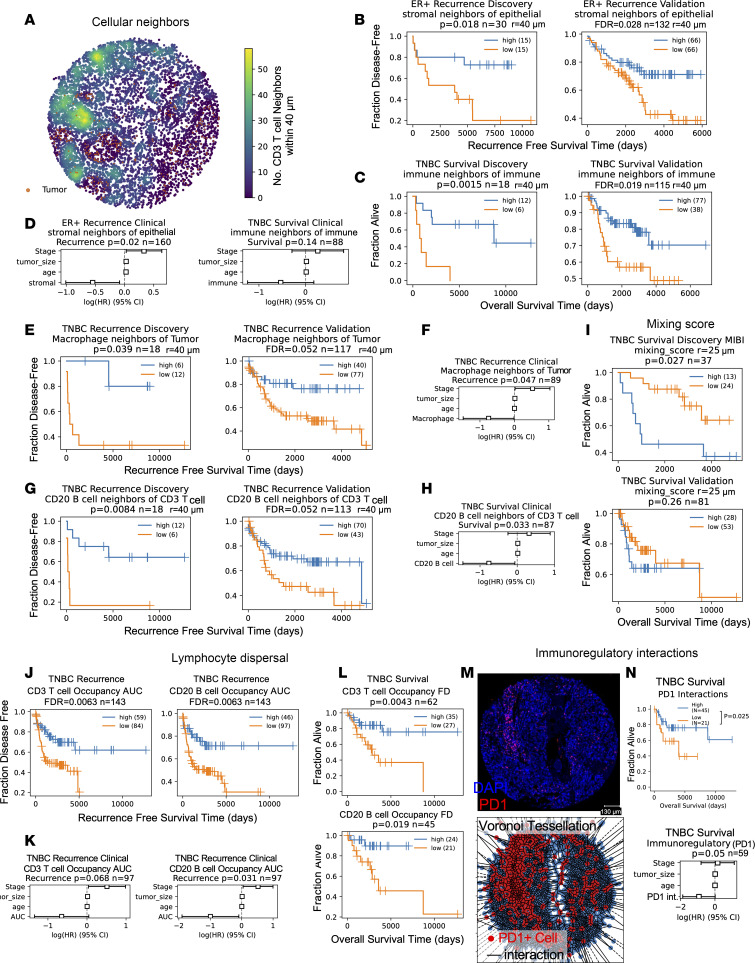
Spatial profiling of tissues promises to elucidate tumor-microenvironment interactions and generate prognostic and predictive biomarkers. We analyzed single-cell spatial data from 3 multiplex imaging technologies: cyclic immunofluorescence (CycIF) data we generated from 102 patients with breast cancer with clinical follow-up as well as publicly available mass cytometry and multiplex ion-beam imaging datasets. Similar single-cell phenotyping results across imaging platforms enabled combined analysis of epithelial phenotypes to delineate prognostic subtypes among patients who are estrogen-receptor+ (ER+). We utilized discovery and validation cohorts to identify biomarkers with prognostic value. Increased lymphocyte infiltration was independently associated with longer survival in triple-negative (TN) and high-proliferation ER+ breast tumors. An assessment of 10 spatial analysis methods revealed robust spatial biomarkers. In ER+ disease, quiescent stromal cells close to tumor were abundant in tumors with good prognoses, while tumor cell neighborhoods containing mixed fibroblast phenotypes were enriched in poor-prognosis tumors. In TN disease, macrophage/tumor and B/T lymphocyte neighbors were enriched, and lymphocytes were dispersed in good-prognosis tumors, while tumor cell neighborhoods containing vimentin+ fibroblasts were enriched in poor-prognosis tumors. In conclusion, we generated comparable single-cell spatial proteomic data from several clinical cohorts to enable prognostic spatial biomarker identification and validation.
Keywords: Breast cancer; Immunology; Macrophages; Oncology; T cells.
Conflict of interest statement
Figures




References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
