

Large clones of clonal hematopoiesis affect outcome in mantle cell lymphoma: results from the FIL MCL0208 clinical trial
- PMID: 39808795
- PMCID: PMC12008534
- DOI: 10.1182/bloodadvances.2024014948
Large clones of clonal hematopoiesis affect outcome in mantle cell lymphoma: results from the FIL MCL0208 clinical trial
Abstract
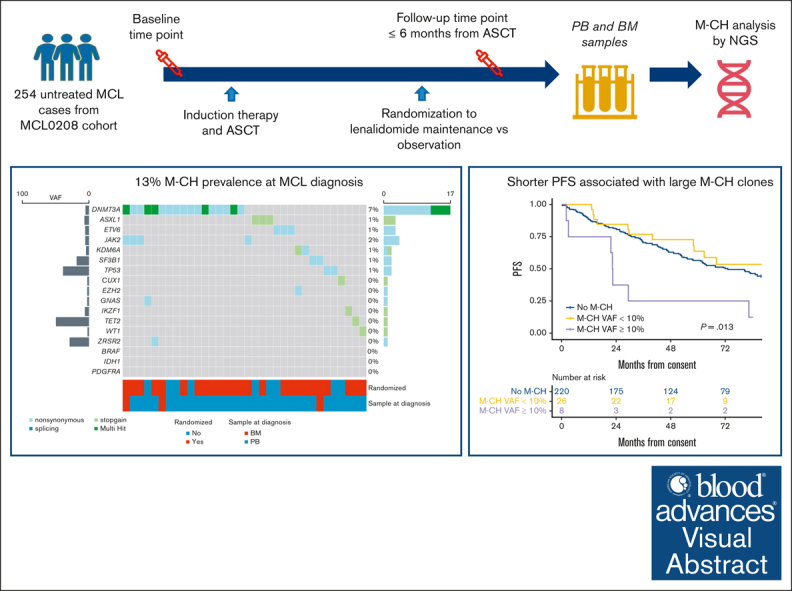
Although recent evidence suggests that myeloid clonal hematopoiesis (M-CH) may influence lymphoma clinical outcome, its impact in mantle cell lymphoma (MCL) remains unclear. Here, we report a comprehensive next-generation sequencing-based analysis of the M-CH mutational landscape at baseline and follow-up in patients enrolled in the Fondazione Italiana Linfomi MCL0208 phase 3 trial, evaluating lenalidomide maintenance vs observation after chemoimmunotherapy and autologous stem cell transplantation (ASCT) in untreated young patients with MCL. Overall, 254 of 300 (85%) enrolled patients (median age, 57 years [range, 32-66]) had a baseline sample available for CH analysis. Using stringent criteria, at least 1 mutation involving M-CH candidate genes was described in 34 patients (13%), with DNMT3A being the most frequently mutated gene (54%). After a median follow-up of 7 years, the presence of large CH clones (variant allele frequency of ≥10%) predicted worse progression-free survival (hazard ratio [HR], 2.93; 95% confidence interval [CI] 1.36-6.31; P = .006) and overall survival (HR, 3.02 [1.21-7.55]; P = .018) compared with patients with CH. Importantly, the competing risks analysis demonstrates that the worse clinical outcome associated with M-CH large clones is linked to MCL progression (P < .05). Moreover, large M-CH clones showed longer time to hematological recovery after ASCT than the remaining cohort (P = .026). In conclusion, we showed for the first time that large CH clones might associate with unfavorable clinical impact in patients with MCL. This trial was registered at www.clinicaltrialsregister.eu as EudraCT (2009-012807-25) and www.ClinicalTrials.gov as #NCT02354313.
© 2025 American Society of Hematology. Published by Elsevier Inc. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: V.R.Z. serves on the advisory board of Kite/Gilead and Takeda; is a consultant for Roche; received research funding from Kite/Gilead; is a member of the speakers bureau for Janssen, Lilly, and Takeda; and received travel support from BeiGene, Janssen, Roche, and Takeda. M.G.d.S. received research grants from Gilead Sciences and AstraZeneca; serves on the advisory board of Janssen, Roche, Gilead Sciences, Lilly, and Takeda; received institutional payments from Janssen and AbbVie; and received travel support from Roche, AbbVie, Janssen, Gilead, and Takeda. M.L. reports consulting fees from AstraZeneca, BeiGene, Janssen, and Lilly; reports honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from AstraZeneca, BeiGene, Janssen, and Lilly; and reports participation on a data safety monitoring board with Acerta. S.F. is a consultant for Janssen, EUSA Pharma, AbbVie, and Sandoz; serves on the advisory board of Janssen, EUSA Pharma, Recordati, Incyte, Roche, Astra Zeneca, and Italfarmaco; received speaker’s honoraria from Janssen, EUSA Pharma, Recordati, Lilly, BeiGene, Gilead, and Gentili; and received research funding from Gilead, BeiGene, and Morphosys. E.R. owns shares in enGenome s.r.l. The remaining authors declare no competing financial interests.
Figures




References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
