

A high fraction of inspired oxygen does not mitigate atelectasis-induced lung tissue hypoxia or injury in experimental acute respiratory distress syndrome
- PMID: 39809828
- PMCID: PMC11733249
- DOI: 10.1038/s41598-024-83992-2
A high fraction of inspired oxygen does not mitigate atelectasis-induced lung tissue hypoxia or injury in experimental acute respiratory distress syndrome
Abstract
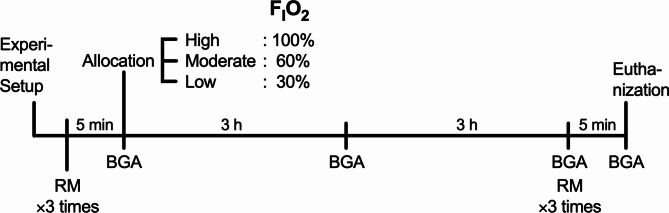
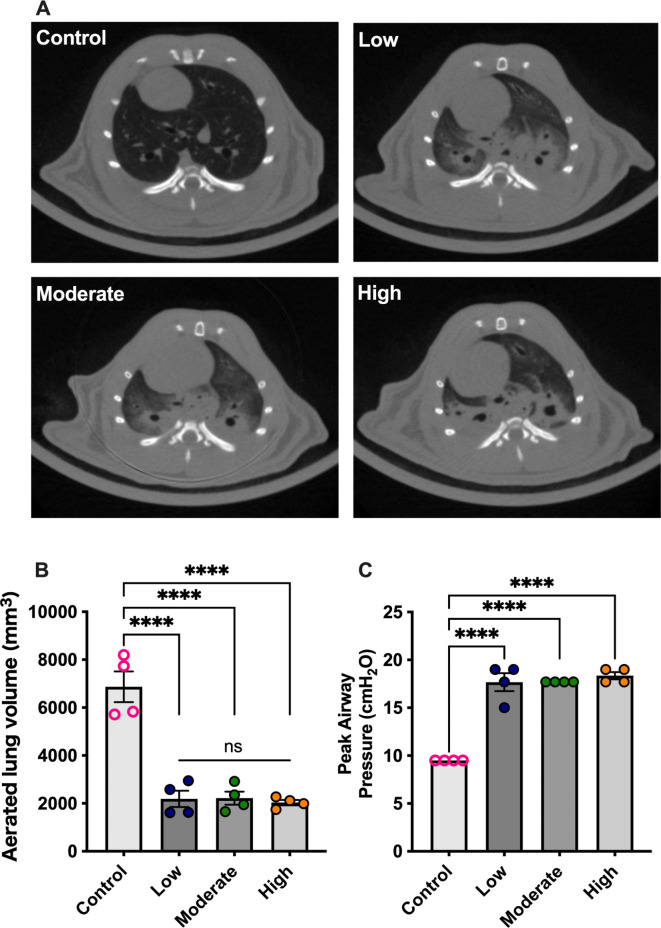
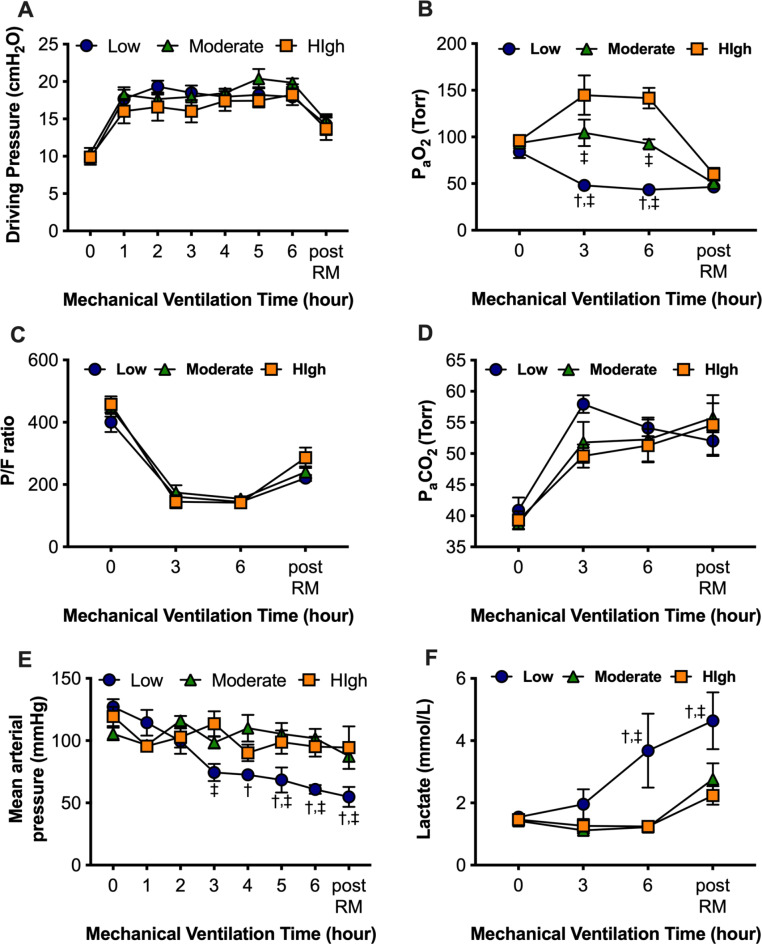
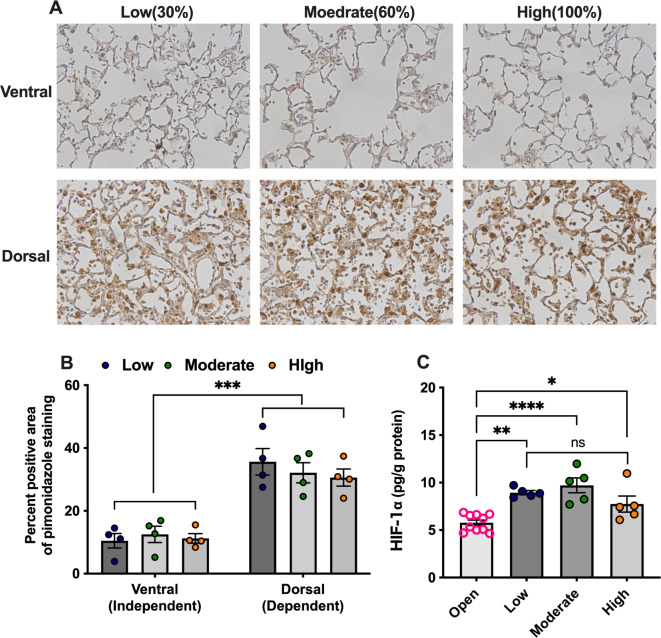
Although alveolar hyperoxia exacerbates lung injury, clinical studies have failed to demonstrate the beneficial effects of lowering the fraction of inspired oxygen (FIO2) in patients with acute respiratory distress syndrome (ARDS). Atelectasis, which is commonly observed in ARDS, not only leads to hypoxemia but also contributes to lung injury through hypoxia-induced alveolar tissue inflammation. Therefore, it is possible that excessively low FIO2 may enhance hypoxia-induced inflammation in atelectasis, and raising FIO2 to an appropriate level may be a reasonable strategy for its mitigation. In this study, we investigated the effects of different FIO2 levels on alveolar tissue hypoxia and injury in a mechanically ventilated rat model of experimental ARDS with atelectasis. Rats were intratracheally injected with lipopolysaccharide (LPS) to establish an ARDS model. They were allocated to the low, moderate, and high FIO2 groups with FIO2 of 30, 60, and 100%, respectively, a day after LPS injection. All groups were mechanically ventilated with an 8 mL/kg tidal volume and zero end-expiratory pressure to induce dorsal atelectatic regions. Arterial blood gas analysis was performed every 2 h. After six hours of mechanical ventilation, the rats were euthanized, and blood, bronchoalveolar lavage fluid, and lung tissues were collected and analyzed. Another set of animals was used for pimonidazole staining of the lung tissues to detect the hypoxic region. Lung mechanics, ratios of partial pressure of arterial oxygen (PaO2) to FIO2, and partial pressure of arterial carbon dioxide were not significantly different among the three groups, although PaO2 changed with FIO2. The dorsal lung tissues were positively stained with pimonidazole regardless of FIO2, and the HIF-1α concentrations were not significantly different among the three groups, indicating that raising FIO2 could not rescue alveolar tissue hypoxia. Moreover, changes in FIO2 did not significantly affect lung injury or inflammation. In contrast, hypoxemia observed in the low FIO2 group caused injury to organs other than the lungs. Raising FIO2 levels did not attenuate tissue hypoxia, inflammation, or injury in the atelectatic lung region in experimental ARDS. Our results indicate that raising FIO2 levels to attenuate atelectasis-induced lung injury cannot be rationalized.
Keywords: Acute respiratory distress syndrome; Alveolar hypoxia; Atelectasis; Hypoxia-induced inflammation; Oxygen.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests. Ethics approval: All experimental animal protocols were reviewed and approved by the Animal Research Committee of Yokohama City University, Japan. Consent to participate: Not applicable.
Figures



References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
