

Review
doi: 10.1007/s00428-024-04011-3.
Epub 2025 Jan 15.
Congenital melanocytic neoplasms: clinical, histopathological and recent molecular developments
Affiliations
- PMID: 39810001
- PMCID: PMC11782411
- DOI: 10.1007/s00428-024-04011-3
Item in Clipboard
Review
Congenital melanocytic neoplasms: clinical, histopathological and recent molecular developments
Virchows Arch.
2025 Jan.
No abstract available
Keywords: Congenital nevus; Neurocutaneous melanocytosis; Pediatric melanocytic neoplasm; Pediatric melanoma.
Conflict of interest statement
Declarations. Ethics approval: This article contains deidentified histologic images collected as part of the "The Gavin Bailey Tissue Repository for Neural Crest Disorders", (IRB University of Pittsburgh PRO10030357); Dr. Miguel Reyes-Mugica (PI) and Dr. Claudia Maria Salgado (Co-investigator). All the images are part of the author’s own work. Consent to participate: N/A. Consent for publication: N/A. Conflict of interest: The authors declare no competing interests.
Figures

Clinical figures of patients with CMN with different phenotypes. A Woman with CMN with bolero pattern, occupying the entire upper and middle back region. Note the folds and grooves with redundant tissue, as well as numerous satellite lesions. B Male with CMN located at the right scapular region with marked hypertrichosis. C, D Two children with CMN on the legs are shown, the first with a localized lesion on the ankle with areas of different color and thickness and the second with a uniform brown lesion of moderate thickness
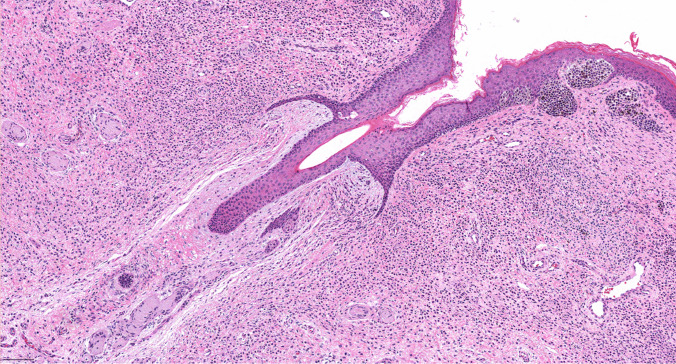
Classical appearance of a congenital melanocytic nevus with a compound architecture (junctional and dermal components), prominent dermal band-like distribution of the lesional cells, infiltration of the skin adnexa and “so-called” neurotization
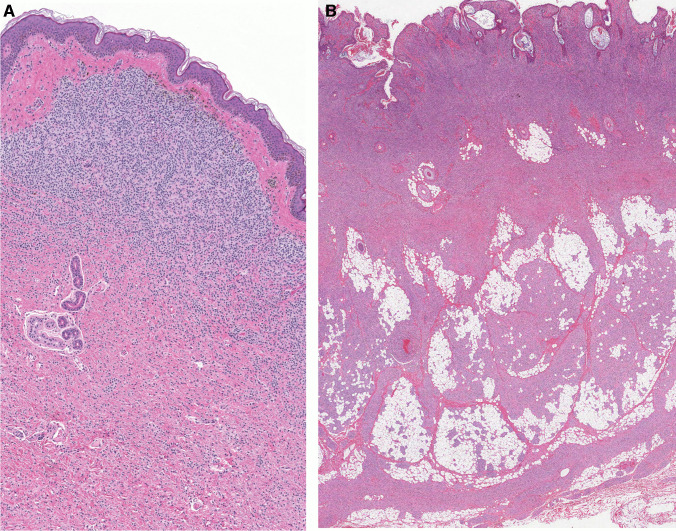
Histologic appearance of congenital melanocytic nevus with a dermal (A) or compound (B) histologic architecture and prominent band-like pattern. A The melanocytic lesion shows no junctional component and a well-defined Grenz zone in the papillary dermis with atrophy of rete ridges. B Lesion with prominent papillomatosis (verrucoid features) and nevomelanocytes in the deep subcutaneous tissue/ fascia
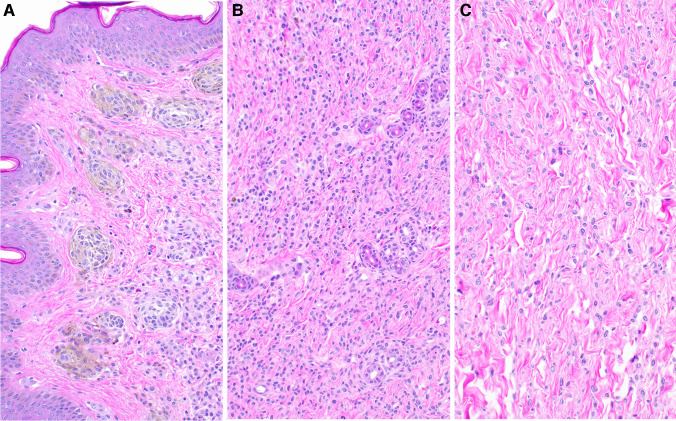
A Superficial area of the lesion composed by more mature nevomelanocytes (type A); larger epithelioid cells with abundant cytoplasm and intracytoplasmic melanin. B Midway through the nevus, it is composed by compact groups of round cells (type B) which appear as single files between collagen bundles infiltrating adnexal structures. C In the deep dermal layers and subcutaneous tissue, the lesional cells are spindly and still immature (type C nevocytes) with a neuroid phenotype (resembling their nerve-sheath based predecessors, the Schwann-cell precursors), poorly defined cytoplasm and limited pigmentation
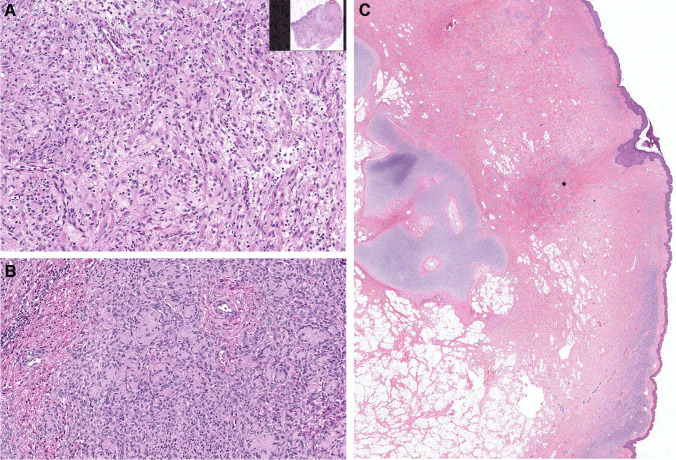
Recapitulating their presumed neural crest origin, nevus cells can show aberrant lines of differentiation. (A) CMN with a nodular lesion showing neufibroma-like appearance with few ganglion cells. (B) A schwannoma-like pattern in the form of Wegner-Meissner or Masson bodies. (C) Represents a CMN with hamartomatous appearance, excess adipose tissue and other mesenchymal elements, including cartilage and aberrant vasculature
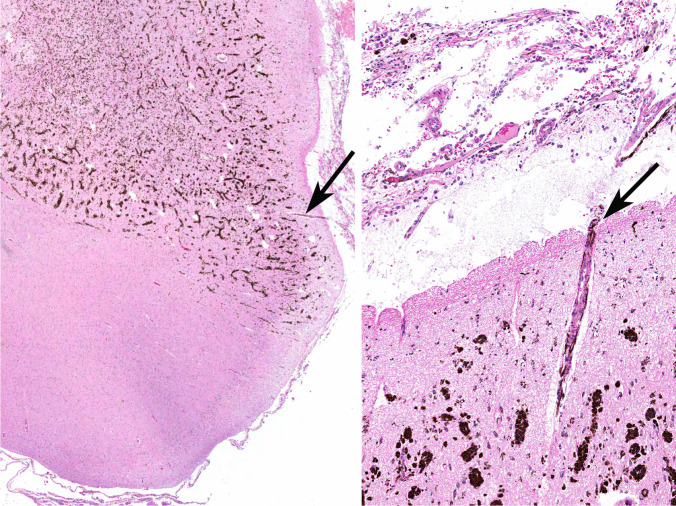
Representative images of a 9 year-old patient with NCM. Left: low power view of the hippocampus heavily pigmented nevomelanocytes infiltrating the central nervous system parenchyma in a predominantly perivascular pattern. Right: slightly higher magnification showing the same blood vessel with its perivascular Virchow-Robin space populated by invading nevomelanocytes which infiltrate the brain parenchyma. Observe the overlying leptomeninges with the heavily pigmented proliferating nevomelanocytes. The arrows in both frames point to the same blood vessel
Similar articles
-
Large congenital melanocytic nevi and the risk for development of malignant melanoma and neurocutaneous melanocytosis.Pediatrics. 2000 Oct;106(4):736-41. doi: 10.1542/peds.106.4.736. Pediatrics. 2000. PMID: 11015516
-
Congenital melanocytic nevi: treatment modalities and management options.Semin Cutan Med Surg. 2003 Mar;22(1):21-32. doi: 10.1053/sder.2003.50002. Semin Cutan Med Surg. 2003. PMID: 12773011 Review.
-
Congenital melanocytic naevi.Australas J Dermatol. 2009 Nov;50(4):231-40; quiz 241-2. doi: 10.1111/j.1440-0960.2009.00553_1.x. Australas J Dermatol. 2009. PMID: 19916964 Review.
-
Giant congenital melanocytic nevi: the significance of neurocutaneous melanosis in neurologically asymptomatic children.Plast Reconstr Surg. 2001 Apr 1;107(4):933-41. doi: 10.1097/00006534-200104010-00005. Plast Reconstr Surg. 2001. PMID: 11252085
-
Giant congenital melanocytic nevus.An Bras Dermatol. 2013 Nov-Dec;88(6):863-78. doi: 10.1590/abd1806-4841.20132233. An Bras Dermatol. 2013. PMID: 24474093 Free PMC article. Review.
Cited by
-
Congenital Melanocytic Nevus with Neurocristic Cutaneous Hamartoma: A Case Report.Dermatopathology (Basel). 2025 Apr 10;12(2):12. doi: 10.3390/dermatopathology12020012. Dermatopathology (Basel). 2025. PMID: 40265343 Free PMC article.
References
-
- Salgado CM, Reyes-Múgica M, Adameyko I, Etchevers HC, Singh R (2022) Congenital naevi. In: WHO Classification of Tumours Editorial Board (eds) Paediatric tumours. WHO classification of tumours series, 5th edn, vol 7. International Agency for Research on Cancer, Lyon. Available from: https://tumourclassificationiarcwhoint/. Accessed 17 Jul 2024
-
- Krengel S, Scope A, Dusza SW, Vonthein R, Marghoob AA (2013) New recommendations for the categorization of cutaneous features of congenital melanocytic nevi. J Am Acad Dermatol 68(3):441–451 - PubMed
-
- Alper JC, Holmes LB (1983) The incidence and significance of birthmarks in a cohort of 4,641 newborns. Pediatr Dermatol 1(1):58–68 - PubMed
-
- Chaithirayanon S, Chunharas A (2013) A survey of birthmarks and cutaneous skin lesions in newborns. J Med Assoc Thai 96(Suppl 1):S49-53 - PubMed
-
- Castilla EE, da Graca Dutra M, Orioli-Parreiras IM (1981) Epidemiology of congenital pigmented naevi: I. Incidence rates and relative frequencies. Br J Dermatol. 104(3):307–15. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
