

Outcome of Patients Transplanted for C3 Glomerulopathy and Primary Immune Complex-Mediated Membranoproliferative Glomerulonephritis
- PMID: 39810762
- PMCID: PMC11725970
- DOI: 10.1016/j.ekir.2024.10.008
Outcome of Patients Transplanted for C3 Glomerulopathy and Primary Immune Complex-Mediated Membranoproliferative Glomerulonephritis
Abstract
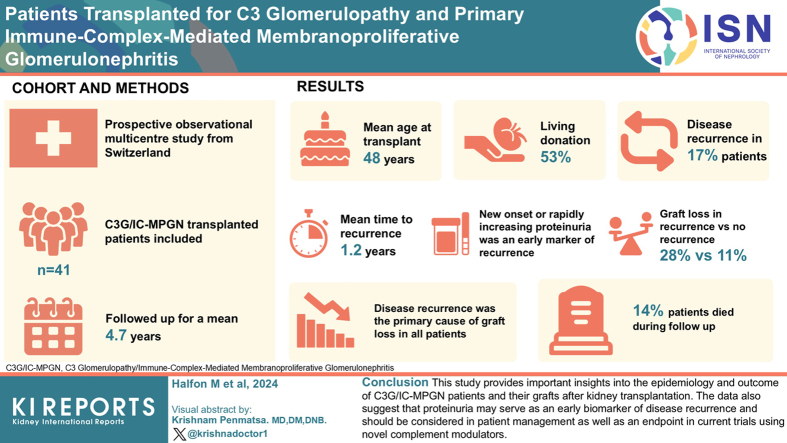
Introduction: Approximately 50% of patients with C3 glomerulopathy (C3G) and primary immune complex-mediated membranoproliferative glomerulonephritis (IC-MPGN) reach kidney failure 10 years after diagnosis. Because these patients are generally young, the majority will be listed for kidney transplantation (KTx). However, reported outcomes in patients transplanted for C3G and IC-MPGN are heterogeneous and conflicting, because they are mainly based on retrospective monocentric studies. We thus aimed to provide detailed multicenter data on these patients, taking advantage of the ongoing nationwide Swiss Transplant Cohort Study (STCS).
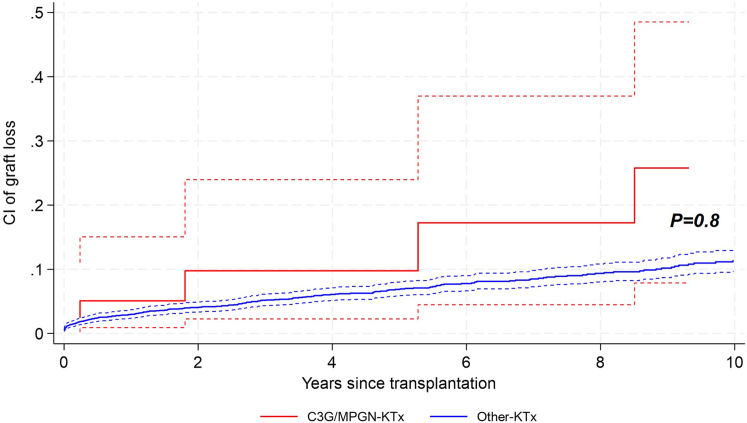
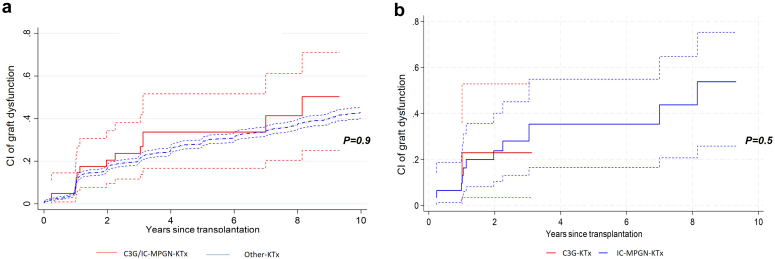
Methods: We analyzed patient and graft outcomes, including the risk of graft loss in relation to recurrence of glomerulopathy.
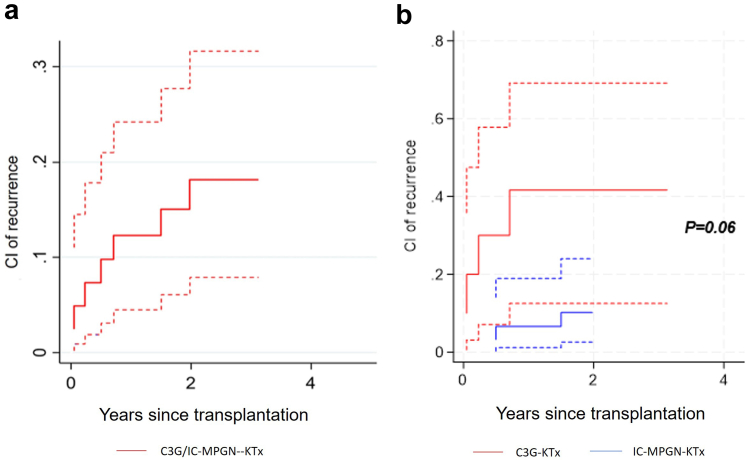
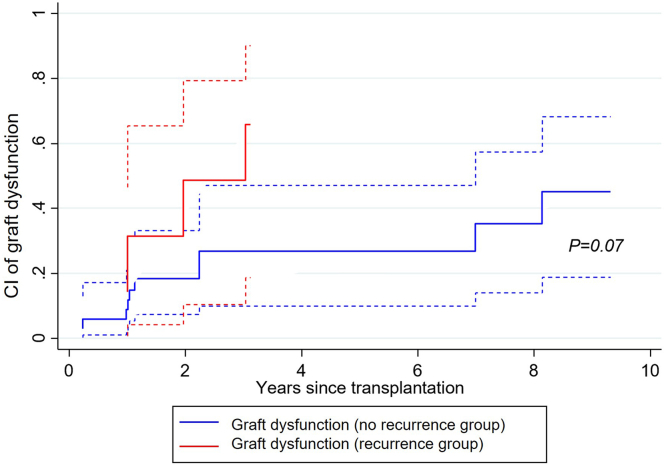
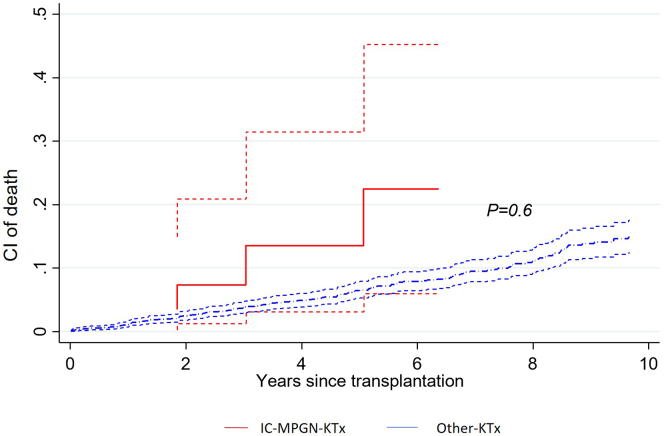
Results: Forty-one (10 C3G and 31 IC-MPGN) transplanted recipients were included with a mean age at transplantation of 48 ± 16 years. Living donors provided 53% of the organs. During a mean follow-up of 4.7 years, 7 patients (4 C3G and 3 IC-MPGN) presented disease recurrence with a mean time to recurrence of 1.2 years. New-onset or rapidly increasing proteinuria was an early marker of recurrence, preceding significant decline in estimated glomerular filtration rate (eGFR). Following recurrence, 28% lost their graft, compared to 11% of patients without recurrence. Disease recurrence was the primary cause of graft loss in all patients. Finally, 14% of patients died during follow-up.
Conclusion: This study provides important insights into the epidemiology and outcome of patients with C3G and IC-MPGN and their grafts after KTx. The data also suggest that proteinuria may serve as an early biomarker of disease recurrence and should be considered in patient management as well as an endpoint in current clinical trials using novel complement modulators.
Keywords: C3 glomerulopathy; cohort study; complement pathway; graft outcome; kidney transplantation; membranoproliferative glomerulonephritis.
© 2024 International Society of Nephrology. Published by Elsevier Inc.
Figures

Comment in
-
Anticomplement Therapies for C3 Glomerulopathy and Immune-Complex Membranoproliferative Glomerulonephritis Recurrence - A Dawn of New Hope.Kidney Int Rep. 2024 Nov 19;10(1):7-9. doi: 10.1016/j.ekir.2024.11.018. eCollection 2025 Jan. Kidney Int Rep. 2024. PMID: 39812304 Free PMC article. No abstract available.
References
-
- Lomax-Browne H.J., Medjeral-Thomas N.R., Barbour S.J., et al. Association of histologic parameters with outcome in C3 glomerulopathy and idiopathic immunoglobulin-associated membranoproliferative glomerulonephritis. Clin J Am Soc Nephrol. 2022;17:994–1007. doi: 10.2215/CJN.16801221. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
