

Prognostic model for esophagogastric variceal rebleeding after endoscopic treatment in liver cirrhosis: A Chinese multicenter study
- PMID: 39811510
- PMCID: PMC11684194
- DOI: 10.3748/wjg.v31.i2.100234
Prognostic model for esophagogastric variceal rebleeding after endoscopic treatment in liver cirrhosis: A Chinese multicenter study
Abstract
Background: Rebleeding after recovery from esophagogastric variceal bleeding (EGVB) is a severe complication that is associated with high rates of both incidence and mortality. Despite its clinical importance, recognized prognostic models that can effectively predict esophagogastric variceal rebleeding in patients with liver cirrhosis are lacking.
Aim: To construct and externally validate a reliable prognostic model for predicting the occurrence of esophagogastric variceal rebleeding.
Methods: This study included 477 EGVB patients across 2 cohorts: The derivation cohort (n = 322) and the validation cohort (n = 155). The primary outcome was rebleeding events within 1 year. The least absolute shrinkage and selection operator was applied for predictor selection, and multivariate Cox regression analysis was used to construct the prognostic model. Internal validation was performed with bootstrap resampling. We assessed the discrimination, calibration and accuracy of the model, and performed patient risk stratification.
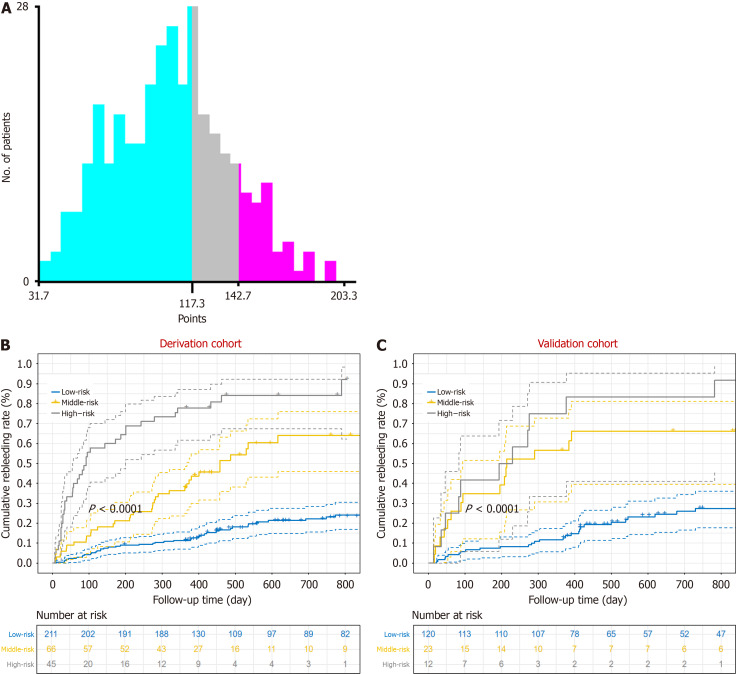
Results: Six predictors, including albumin and aspartate aminotransferase concentrations, white blood cell count, and the presence of ascites, portal vein thrombosis, and bleeding signs, were selected for the rebleeding event prediction following endoscopic treatment (REPET) model. In predicting rebleeding within 1 year, the REPET model exhibited a concordance index of 0.775 and a Brier score of 0.143 in the derivation cohort, alongside 0.862 and 0.127 in the validation cohort. Furthermore, the REPET model revealed a significant difference in rebleeding rates (P < 0.01) between low-risk patients and intermediate- to high-risk patients in both cohorts.
Conclusion: We constructed and validated a new prognostic model for variceal rebleeding with excellent predictive performance, which will improve the clinical management of rebleeding in EGVB patients.
Keywords: Esophagogastric variceal bleeding; Liver cirrhosis; Prognostic model; Risk stratification; Secondary prophylaxis; Variceal rebleeding.
©The Author(s) 2025. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All the authors report no relevant conflicts of interest for this article.
Figures




Similar articles
-
Limitations and enhancement opportunities for variceal rebleeding prediction model in patients with cirrhosis.World J Gastroenterol. 2025 Feb 28;31(8):102841. doi: 10.3748/wjg.v31.i8.102841. World J Gastroenterol. 2025. PMID: 40062338 Free PMC article.
-
Predicting early rebleeding and mortality after endoscopic hemostasis of esophagogastric varices: Diagnostic performance of aspartate aminotransferase-to-platelet ratio index and model for end-stage liver disease-Na score.J Hepatobiliary Pancreat Sci. 2024 Nov;31(11):830-839. doi: 10.1002/jhbp.12057. Epub 2024 Jul 18. J Hepatobiliary Pancreat Sci. 2024. PMID: 39022894
-
[Outcomes of Endoscopic Treatment of Esophagogastric Variceal Bleeding and Construction and Validation of a 1-Year Rebleeding Risk Prediction Model].Sichuan Da Xue Xue Bao Yi Xue Ban. 2025 Jan 20;56(1):284-290. doi: 10.12182/20250160106. Sichuan Da Xue Xue Bao Yi Xue Ban. 2025. PMID: 40109450 Free PMC article. Chinese.
-
Endoscopic treatment of esophageal varices in patients with liver cirrhosis.World J Gastroenterol. 2014 Sep 28;20(36):13015-26. doi: 10.3748/wjg.v20.i36.13015. World J Gastroenterol. 2014. PMID: 25278695 Free PMC article. Review.
-
Variceal and other portal hypertension related bleeding.Best Pract Res Clin Gastroenterol. 2013 Oct;27(5):649-64. doi: 10.1016/j.bpg.2013.08.004. Epub 2013 Sep 5. Best Pract Res Clin Gastroenterol. 2013. PMID: 24160925 Review.
Cited by
-
Limitations and enhancement opportunities for variceal rebleeding prediction model in patients with cirrhosis.World J Gastroenterol. 2025 Feb 28;31(8):102841. doi: 10.3748/wjg.v31.i8.102841. World J Gastroenterol. 2025. PMID: 40062338 Free PMC article.
-
Development and validation of machine learning models to predict esophagogastric variceal rebleeding risk in HBV-related cirrhosis after endoscopic treatment: a prospective multicenter study.EClinicalMedicine. 2025 Aug 20;87:103436. doi: 10.1016/j.eclinm.2025.103436. eCollection 2025 Sep. EClinicalMedicine. 2025. PMID: 40896458 Free PMC article.
References
-
- Garcia-Tsao G, Abraldes JG, Berzigotti A, Bosch J. Portal hypertensive bleeding in cirrhosis: Risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the study of liver diseases. Hepatology. 2017;65:310–335. - PubMed
-
- Yang J, Ge K, Chen L, Yang JL. The efficacy comparison of carvedilol plus endoscopic variceal ligation and traditional, nonselective β-blockers plus endoscopic variceal ligation in cirrhosis patients for the prevention of variceal rebleeding: a meta-analysis. Eur J Gastroenterol Hepatol. 2019;31:1518–1526. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
