

Tranexamic acid for preventing postpartum haemorrhage after vaginal birth
- PMID: 39812173
- PMCID: PMC12043208
- DOI: 10.1002/14651858.CD007872.pub4
Tranexamic acid for preventing postpartum haemorrhage after vaginal birth
Abstract
Rationale: Postpartum haemorrhage (PPH) is common and potentially life-threatening. The antifibrinolytic drug tranexamic acid (TXA) is thought to be effective for treating PPH. There is growing interest in whether TXA is effective for preventing PPH after vaginal birth. In randomised controlled trials (RCTs), TXA has been associated with increased risk of seizures and unexplained increased mortality when given more than three hours after traumatic bleeding. Reliable evidence on the effects, cost-effectiveness and safety of prophylactic TXA is required before considering widespread use. This review updates one published in 2015.
Objectives: To assess the effects of TXA for preventing PPH compared to placebo or no treatment (with or without uterotonic co-treatment) in women following vaginal birth.
Search methods: We searched MEDLINE, Embase, CENTRAL, and WHO ICTRP (to 6 September 2024). We also searched reference lists of retrieved studies.
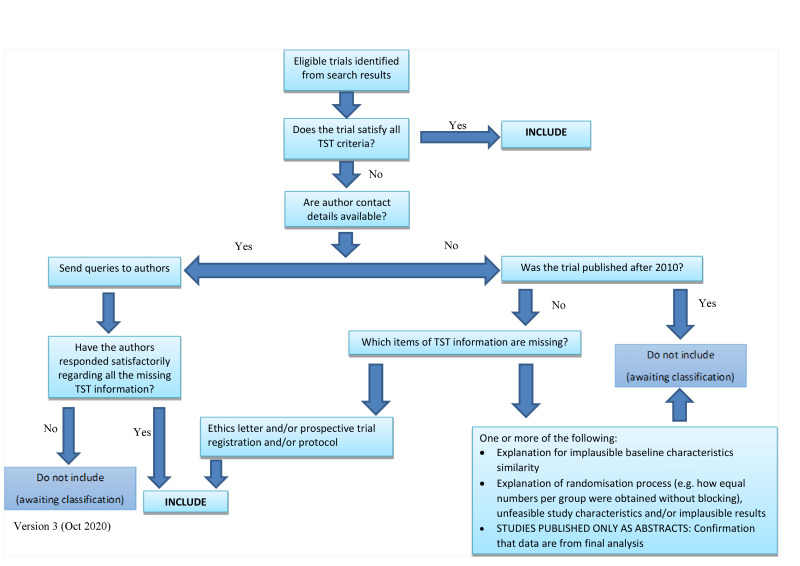
Eligibility criteria: We included RCTs evaluating TXA alone or in addition to standard care (uterotonics) for preventing PPH following vaginal birth. For this update, we required trials to be prospectively registered (before participant recruitment), and we applied a trustworthiness checklist.
Outcomes: Critical outcomes were blood loss ≥ 500 mL and blood loss ≥ 1000 mL. Important outcomes included maternal death, severe morbidity, blood transfusion, receipt of additional surgical interventions to control PPH, thromboembolic events, receipt of additional uterotonics, hysterectomy, and maternal satisfaction.
Risk of bias: We used the Cochrane risk of bias tool (RoB 1) to assess the risk of bias in the studies.
Synthesis methods: Two review authors independently selected trials, extracted data, assessed risk of bias, and assessed trial trustworthiness. We used random-effects meta-analysis to combine data. We assessed the certainty of the evidence using GRADE.
Included studies: We included three RCTs with 18,974 participants in total. The trials were conducted in both high- and low-resource settings and involved participants at both low and high risk of PPH. The trials compared intravenous TXA (1 g) and standard care versus placebo (saline) and standard care. After applying our trustworthiness checklist, we did not include any of the 12 trials in the previous version of this review.
Synthesis of results: Prophylactic tranexamic acid in addition to standard care compared to placebo in addition to standard care TXA results in little to no difference in blood loss ≥ 500 mL (risk ratio (RR) 0.93, 95% confidence interval (CI) 0.81 to 1.06; 2 studies, 18,897 participants; 5 fewer per 1000, 95% CI 15 fewer to 5 more; high-certainty evidence). TXA likely results in little to no difference in blood loss ≥ 1000 mL (RR 0.86, 95% CI 0.69 to 1.07; 2 studies, 18,897 participants; 3 fewer per 1000, 95% CI 6 fewer to 1 more; moderate-certainty evidence). TXA likely results in little to no difference in severe morbidity (RR 0.88, 95% CI 0.69 to 1.12; 1 study, 15,066 participants; 2 fewer per 1000, 95% CI 6 fewer to 2 more; moderate-certainty evidence). TXA results in little to no difference in receipt of blood transfusion (RR 1.00, 95% CI 0.95 to 1.06; 3 studies, 18,972 participants; 0 fewer per 1000, 95% CI 10 fewer to 12 more; high-certainty evidence). TXA may result in little to no difference in receipt of additional surgical interventions to control PPH (RR 0.63, 95% CI 0.32 to 1.23; 2 studies, 18,972 participants; 1 fewer per 1000, 95% CI 2 fewer to 1 more; low-certainty evidence). In women with anaemia, TXA results in little to no difference in receipt of additional uterotonics (RR 1.02, 95% CI 0.94 to 1.10; 1 study, 15,066 participants; 3 more women per 1000, 95% CI 8 fewer to 24 more; high-certainty evidence). In women with no anaemia, TXA results in a slight reduction in receipt of additional uterotonics (RR 0.75, 95% CI 0.61 to 0.92; 1 study, 3891 participants; 24 fewer women per 1000, 95% CI 38 fewer to 8 fewer; high-certainty evidence). TXA likely results in little to no difference in maternal satisfaction. The evidence is very uncertain about the effect of TXA on maternal death, thromboembolic events, and hysterectomy (very low-certainty evidence): maternal death (RR 0.99, 95% CI 0.39 to 2.49; 2 studies, 15,081 participants; 0 fewer per 1000, 95% CI 1 fewer to 2 more); thromboembolic events (RR 0.25, 95% CI 0.03 to 2.24; 3 studies, 18,774 participants; 3 fewer women per 10,000, 95% CI 4 fewer to 5 more); hysterectomy (RR 0.89, 95% CI 0.36 to 2.19; 1 study, 15,066 participants; 1 fewer women per 10,000, 95% CI 9 fewer to 16 more).
Authors' conclusions: Adding prophylactic TXA to standard care of women during vaginal birth makes little to no difference to blood loss ≥ 500 mL and likely makes little to no difference to blood loss ≥ 1000 mL or the risk of severe morbidity, compared to placebo and standard care. TXA may result in little to no difference in additional surgical interventions to control PPH and results in little to no difference in blood transfusions. One trial found that TXA reduced the use of additional uterotonics in women without anaemia, whereas the largest trial found little to no difference in the use of additional uterotonics in women with anaemia. Although there were very few serious adverse events reported, the evidence is insufficient to draw conclusions about the effect of TXA on maternal death, thromboembolic events, hysterectomy, or seizures. TXA likely results in little to no difference in maternal satisfaction. These findings are based mainly on two large trials. In the smaller of these, less than 30% of study participants were at high risk of PPH. In the largest trial, all participants had moderate to severe anaemia. Those making decisions about routine administration of prophylactic TXA for all women having vaginal births should consider that current evidence does not show a benefit of TXA for blood loss outcomes and related morbidity, and the evidence is very uncertain about serious adverse events.
Funding: This review was partially funded by the World Health Organization (WHO).
Registration: Protocol (2009) DOI: 10.1002/14651858.CD007872 Original review (2010) DOI: 10.1002/14651858.CD007872.pub2 Review update (2015) DOI: 10.1002/14651858.CD007872.pub3.
Copyright © 2025 The Authors. Cochrane Database of Systematic Reviews published by John Wiley & Sons, Ltd. on behalf of The Cochrane Collaboration.
Conflict of interest statement
Christa Rohwer: received financial support from the World Health Organization (WHO) to complete this review.
Anke Rohwer: is an editor with Cochrane Infectious Diseases but was not involved in the editorial process for this review.
Catherine Cluver: none known
Katharine Ker: is an author of the WOMAN‐2 trial (WOMAN‐2 2024) and did not participate in evaluating this trial in the review process.
G Justus Hofmeyr: has consulted for Equalize Health, a not‐for‐profit health technology company, and has done ad hoc consultation on the 'Maternawell Tray' blood loss monitoring device and integrated suction tube uterine tamponade device, for which he received consulting fees. The Maternawell tray is not mentioned in this review. GJH has published academic articles on tranexamic acid in medical journals.
Figures

















Update of
-
Tranexamic acid for preventing postpartum haemorrhage.Cochrane Database Syst Rev. 2015 Jun 16;2015(6):CD007872. doi: 10.1002/14651858.CD007872.pub3. Cochrane Database Syst Rev. 2015. Update in: Cochrane Database Syst Rev. 2025 Jan 15;1:CD007872. doi: 10.1002/14651858.CD007872.pub4. PMID: 26079202 Free PMC article. Updated.
References
-
- Carroli G, Cuesta C, Abalos E, Gulmezoglu AM. Epidemiology of postpartum haemorrhage: a systematic review. Best Practice & Research. Clinical Obstetrics & Gynaecology 2008;22(6):999-1012. - PubMed
-
- Feduniw S, Warzecha D, Szymusik I, Wielgos M. Epidemiology, prevention and management of early postpartum hemorrhage - a systematic review. Ginekologia Polska 2020;91(4):38-44. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials