

Keratoconus in children in Tunisia: Epidemiological, clinical and therapeutic features
- PMID: 39812204
- PMCID: PMC11906247
- DOI: 10.62438/tunismed.v103i1.5361
Keratoconus in children in Tunisia: Epidemiological, clinical and therapeutic features
Abstract
Aim: To report the clinical and therapeutic particularities of pediatric keratoconus (KC).
Methods: Retrospective study focusing on patients aged less than 18 years, presenting with KC and followed in a tertiary reference center in Sfax, Tunisia.
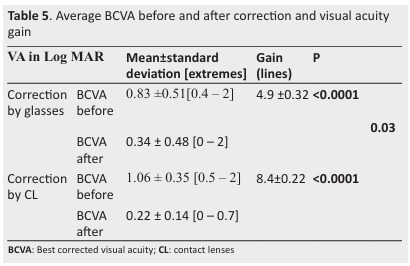
Results: Our study involved 38 eyes of 20 children. We found a mean age of 12.8 years, a family history of keratoconus for 25% of cases and an atopic background in 30% of children. The mean best-corrected visual acuity was 5.3/10, the mean myopia was -6.3D and the mean total astigmatism was -4.9D. The average maximum simulated keratometry (Kmax) was 54.6 D. The visual acuity decrease was correlated with the presence of corneal opacities, with all keratometric indices except Skewed Radial Axes (SRAX) at 3 and 5 mm, with all elevation parameters and those of pachymetry except the delocalization of the thinnest point. 71.1% of eyes were classified as clinical KC and 47% of eyes were classified as Amlser-Krumeich stage 4. 42.1% of eyes were fitted with glasses and 57.9% with contact lenses. Six patients (10 eyes) underwent cross-linking (CXL). We noted an evolution of the KC for 64.29% of eyes not treated with CXL and a stabilization of 80% of eyes treated with CXL. The difference in follow-up parameters between the two groups was significant.
Conclusion: Pediatric KC is a severe disease, often diagnosed at a late stage. CXL is a safe and effective way to stop the disease.
Keywords: Child; Corneal topography; Cross-linking; Keratoconus.
Figures





Similar articles
-
Keratoconus in pre-teen children: Demographics and clinical profile.Indian J Ophthalmol. 2022 Oct;70(10):3508-3513. doi: 10.4103/ijo.IJO_2579_21. Indian J Ophthalmol. 2022. PMID: 36190036 Free PMC article.
-
Visual, Topographic, and Pachymetric Effects of Pediatric Corneal Collagen Cross-linking.J Pediatr Ophthalmol Strabismus. 2017 Mar 1;54(2):84-89. doi: 10.3928/01913913-20160831-01. Epub 2016 Sep 27. J Pediatr Ophthalmol Strabismus. 2017. PMID: 27668869
-
Corneal Collagen Cross-Linking for Keratoconus in Pediatric Patients-Long-Term Results.Cornea. 2017 Feb;36(2):138-143. doi: 10.1097/ICO.0000000000001102. Cornea. 2017. PMID: 28060058
-
Corneal collagen cross-linking: a review of 1-year outcomes.Eye Contact Lens. 2014 Nov;40(6):345-52. doi: 10.1097/ICL.0000000000000094. Eye Contact Lens. 2014. PMID: 25343263 Review.
-
Transepithelial versus epithelium-off corneal crosslinking for progressive keratoconus.Cochrane Database Syst Rev. 2021 Mar 23;3(3):CD013512. doi: 10.1002/14651858.CD013512.pub2. Cochrane Database Syst Rev. 2021. PMID: 33765359 Free PMC article.
References
-
- Buzzonetti L, Bohringer D, Liskova P, Lang S, Valente P. Keratoconus in Children: A Literature Review. Cornea. 2020;39(12):1592–1598. - PubMed
-
- Rabinowitz YS. Keratoconus. Surv Ophthalmol. 1998;42(4):297–319. - PubMed
-
- Saad A. The Challenges of the Detection of Subclinical Keratoconus at Its Earliest Stage. Int J Keratoconus Ectatic Corneal DiS. 2012;1(1):36–43.
-
- Sandali O, El Sanharawi M, Temstet C, Hamiche T, Galan A, Ghouali W. Fourier-domain optical coherence tomography imaging in keratoconus: a corneal structural classification. Ophthalmology. 2013;120(12):2403–2412. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources