

Efficient and accurate commissioning and quality assurance of radiosurgery beam via prior-embedded implicit neural representation learning
- PMID: 39812551
- PMCID: PMC12082765
- DOI: 10.1002/mp.17617
Efficient and accurate commissioning and quality assurance of radiosurgery beam via prior-embedded implicit neural representation learning
Abstract
Background: Dosimetric commissioning and quality assurance (QA) for linear accelerators (LINACs) present a significant challenge for clinical physicists due to the high measurement workload and stringent precision standards. This challenge is exacerbated for radiosurgery LINACs because of increased measurement uncertainty and more demanding setup accuracy for small-field beams. Optimizing physicists' effort during beam measurements while ensuring the quality of the measured data is crucial for clinical efficiency and patient safety.
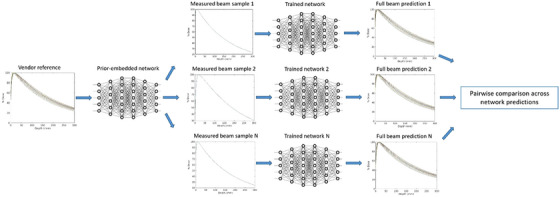
Purpose: To develop a radiosurgery LINAC beam model that embeds prior knowledge of beam data through implicit neural representation (NeRP) learning and to evaluate the model's effectiveness in guiding beam data sampling, predicting complete beam dataset from sparse samples, and verifying detector choice and setup during commissioning and QA.
Materials and methods: Beam data including lateral profile and tissue-phantom-ratio (TPR), collected from CyberKnife LINACs, were investigated. Multi-layer perceptron (MLP) neural networks were optimized to parameterize a continuous function of the beam data, implicitly defined by the mapping from measurement coordinates to measured dose values. Beam priors were embedded into network weights by first training the network to learn the NeRP of a vendor-provided reference dataset. The prior-embedded network was further fine-tuned with sparse clinical measurements and used to predict unacquired beam data. Prospective and retrospective evaluations of different beam data samples in finetuning the model were performed using the reference beam dataset and clinical testing datasets, respectively. Model prediction accuracy was evaluated over 10 clinical datasets collected from various LINACs with different manufacturing modes and collimation systems. Model sensitivity in detecting beam data acquisition errors including inaccurate detector positioning and inappropriate detector choice was evaluated using two additional datasets with intentionally introduced erroneous samples.
Results: Prospective and retrospective evaluations identified consistent beam data samples that are most effective in fine-tuning the model for complete beam data prediction. Despite of discrepancies between clinical beam and the reference beam, fine-tuning the model with sparse beam profile measured at a single depth or with beam TPR measured at a single collimator size predicted beam data that closely match ground truth water tank measurements. Across the 10 clinical beam datasets, the averaged mean absolute error (MAE) in percentage dose was lower than 0.5% and the averaged 1D Gamma passing rate (1%/0.5 mm for profile and 1%/1 mm for TPR) was higher than 99%. In contrast, the MAE and Gamma passing rates were above 1% and below 95% between the reference beam dataset and clinical beam datasets. Model sensitivity to beam data acquisition errors was demonstrated by significant model prediction changes when fine-tuned with erroneous versus correct beam data samples, as quantified by a Gamma passing rate as low as 18.16% between model predictions.
Conclusion: A model for small-field radiosurgery beam was proposed that embeds prior knowledge of beam properties and predicts the entire beam data from sparse measurements. The model can serve as a valuable tool for clinical physicists to verify the accuracy of beam data acquisition and promises to improve commissioning and QA reliability and efficiency with substantially reduced number of beam measurements.
Keywords: beam modeling; machine learning; small field dosimetry.
© 2025 American Association of Physicists in Medicine.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures







References
-
- Tyler M, Liu PZ, Chan KW, et al. Characterization of small‐field stereotactic radiosurgery beams with modern detectors. Phys Med Biol. 2013;58(21):7595. - PubMed
-
- Klein EE, Hanley J, Bayouth J, Yin FF, et al. Task Group 142 report: quality assurance of medical accelerators a. Med Phys. 2009;36(9Part1):4197‐4212. - PubMed
-
- Dieterich S, Cavedon C, Chuang CF, et al. Report of AAPM TG 135: quality assurance for robotic radiosurgery. Med Phys. 2011;38(6Part1):2914‐2936. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
