

Balance recovery and its link to vestibular agnosia in traumatic brain injury: a longitudinal behavioural and neuro-imaging study
- PMID: 39812836
- PMCID: PMC11735511
- DOI: 10.1007/s00415-024-12876-2
Balance recovery and its link to vestibular agnosia in traumatic brain injury: a longitudinal behavioural and neuro-imaging study
Abstract
Background: Vestibular dysfunction causing imbalance affects c. 80% of acute hospitalized traumatic brain injury (TBI) cases. Poor balance recovery is linked to worse return-to-work rates and reduced longevity. We previously showed that white matter network disruption, particularly of right inferior longitudinal fasciculus, mediates the overlap between imbalance and impaired vestibular perception of self-motion (i.e., vestibular agnosia) in acute hospitalized TBI. However, there are no prior reports tracking the acute-longitudinal trajectory of objectively measured vestibular function for hospitalized TBI patients. We hypothesized that recovery of vestibular agnosia and imbalance is linked and mediated by overlapping brain networks.
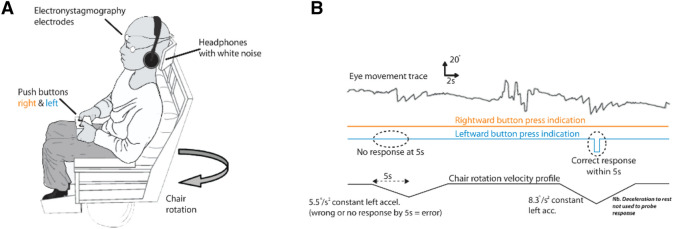
Methods: We screened 918 acute major trauma in-patients, assessed 146, recruited 39 acutely, and retested 34 at 6 months. Inclusion criteria were 18-65-year-old adults hospitalized for TBI with laboratory-confirmed preserved peripheral vestibular function. Benign paroxysmal positional vertigo and migraine were treated prior to testing. Vestibular agnosia was quantified by participants' ability to perceive whole-body yaw plane rotations via an automated rotating-chair algorithm. Subjective symptoms of imbalance (via questionnaires) and objective imbalance (via posturography) were also assessed.
Results: Acute vestibular agnosia predicted poor balance recovery at 6 months. Recovery of vestibular agnosia and linked imbalance was mediated by bihemispheric fronto-posterior cortical circuits. Recovery of subjective symptoms of imbalance and objective imbalance were not correlated.
Conclusion: Vestibular agnosia mediates balance recovery post-TBI. The link between subjective dizziness and brain injury recovery, although important, is unclear. Therapeutic trials of vestibular recovery post-TBI should target enhancing bi-hemispheric connectivity and linked objective clinical measures (e.g., posturography).
Keywords: Diffusion tensor imaging; Imbalance; Resting-state functional connectivity; Self-motion perception; Traumatic brain injury; Vestibular agnosia; Vestibular recovery.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: The authors report no competing interests.
Figures




References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
