

Defining 2 biologically and clinically distinct groups in acute leukemia with a mixed phenotype
- PMID: 39813682
- PMCID: PMC12442034
- DOI: 10.1182/blood.2024026273
Defining 2 biologically and clinically distinct groups in acute leukemia with a mixed phenotype
Abstract
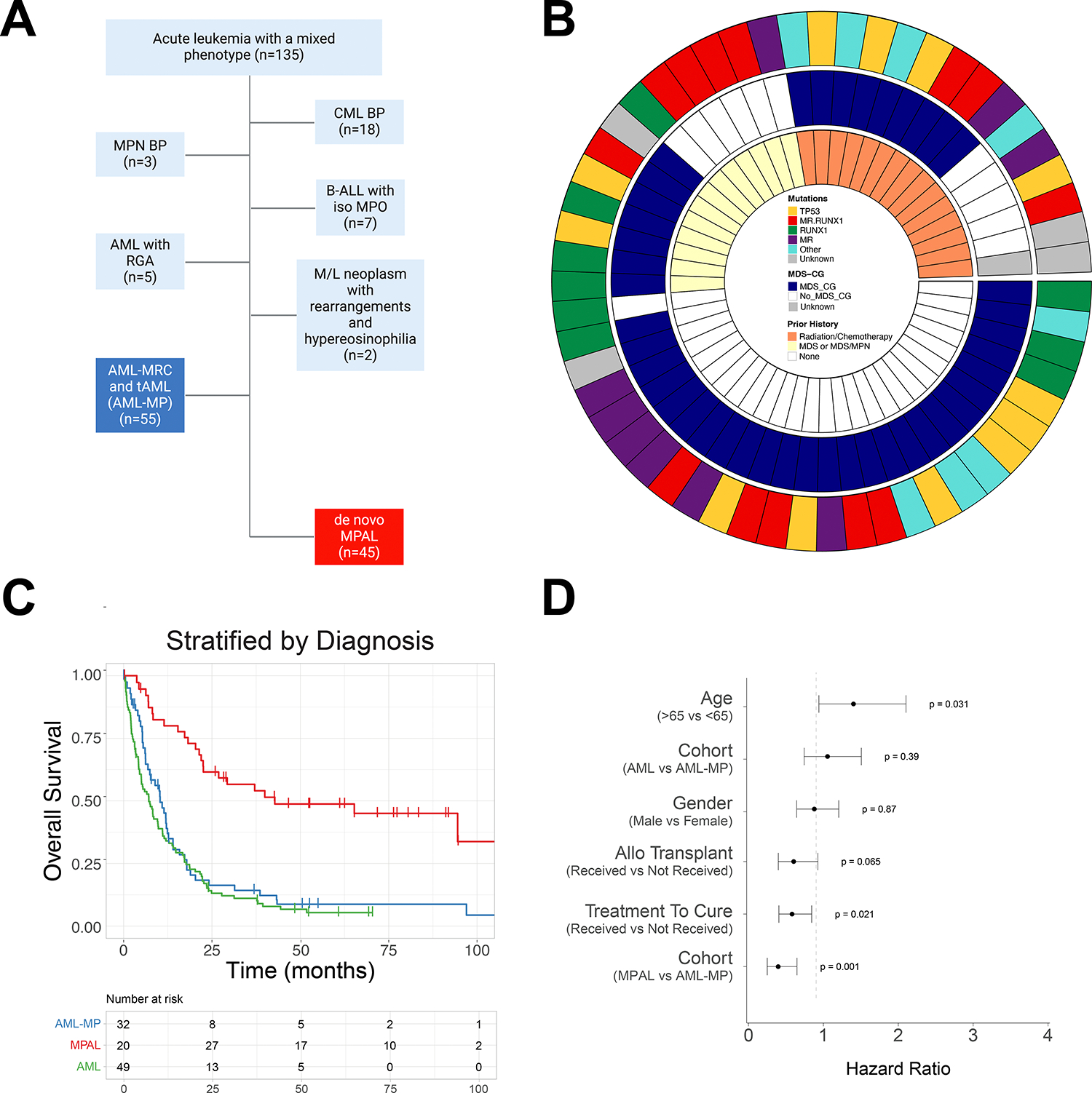
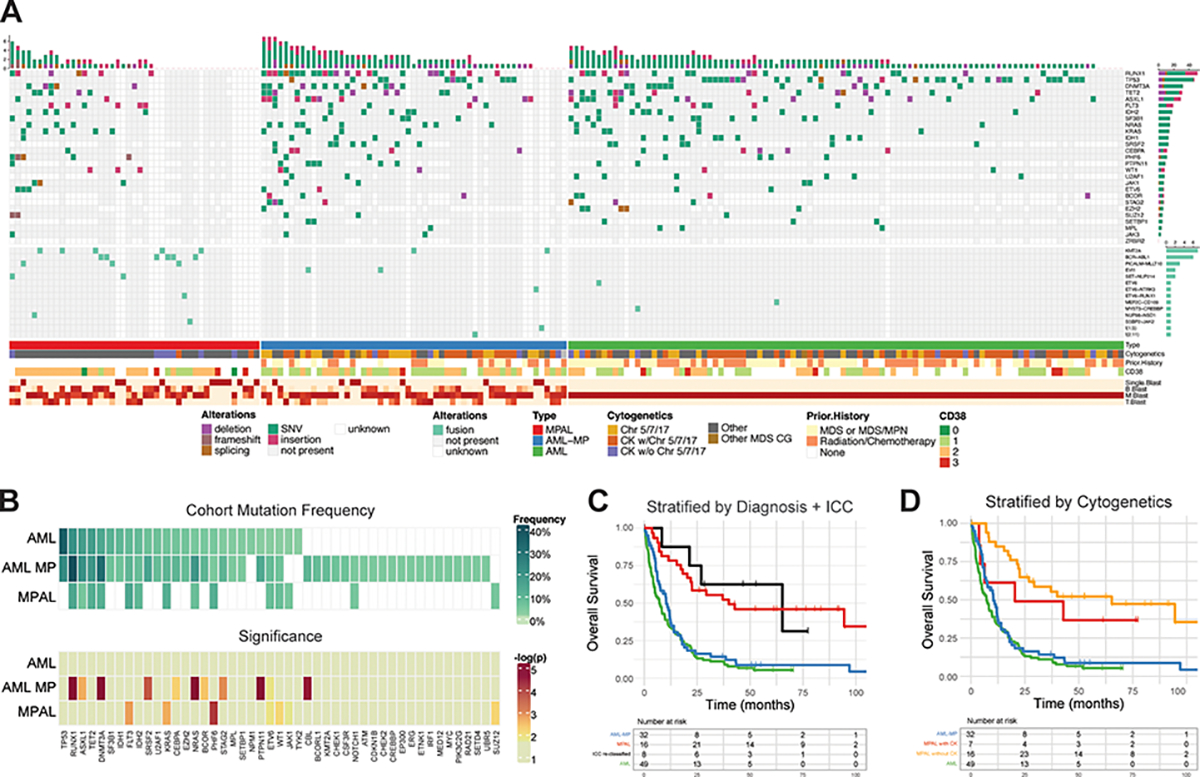
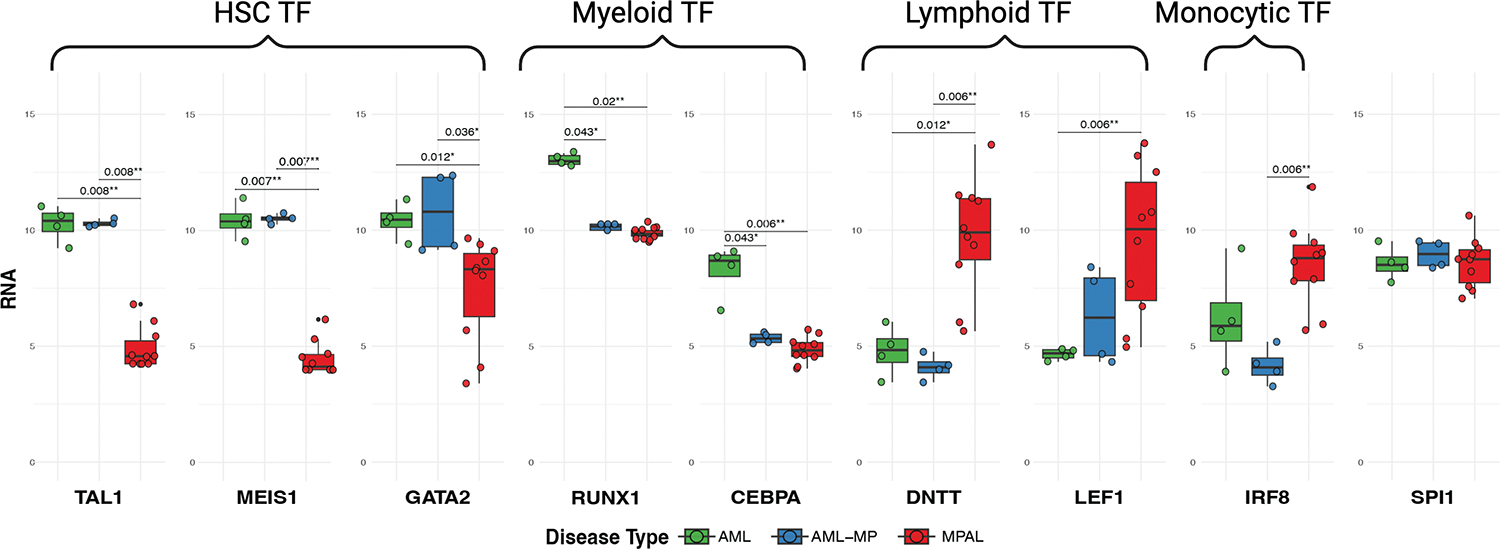
A mixed phenotype (MP) is a characteristic of de novo MP acute leukemia (MPAL), but it can also be found in other leukemias. It poses substantial classification and management dilemmas. Herein, we report a large cohort of acute leukemia with MP and define acute myeloid leukemia with MP (AML-MP) and MPAL as 2 distinct groups by characterizing clinical, genetic, and transcriptomic features. Clinically, patients with AML-MP and MPAL were both treated with either AML- or acute lymphoblastic leukemia (ALL)-directed induction regimens. AML-MP has inferior responses (hazard ratio, 12.5; 95% confidence interval, 2.72-57.8; P = .001), whereas MPAL has better responses to ALL-directed treatment. Genetically, AML-MP harbors more frequent RUNX1 (23/52 [44%]) and TP53 (12/52 [23.1%]) mutations. In contrast, RUNX1 mutations are less frequent in MPAL (8/35 [23%]; P = .01 vs AML-MP) and TP53 mutations as a driver are virtually absent in MPAL. Transcriptionally, AML-MP shows enrichment for stemness signatures and a relative deficit of transcription factors critical for myeloid and lymphoid differentiation. Furthermore, AML-MP rarely switches to a lymphoid immunophenotype after treatment, in contrast to MPAL (1/40 [2.5%] vs 10/28 [35.7%]; P = .0003). Last, a genomic classification framework is proposed for future studies. Together, these data support the designation of AML-MP as a diagnosis distinct from MPAL and provide novel insights into the pathogenesis and therapies of acute leukemia with MP.
© 2025 American Society of Hematology. Published by Elsevier Inc. All rights are reserved, including those for text and data mining, AI training, and similar technologies.
Conflict of interest statement
Conflict of Interest:
M.A served as consultant for Janssen Global Services, Bristol-Myers Squibb, AstraZeneca, and Roche; and has received honoraria from Biocartis, Invivoscribe, physician educational resources (PER), Peerview Institute for medical education, clinical care options, RMEI medical education. RLL is on the supervisory board of Qiagen and is a scientific advisor to Imago, Mission Bio, Syndax. Zentalis, Ajax, Bakx, Auron, Prelude, C4 Therapeutics and Isoplexis for which he receives equity support. RLL receives research support from Ajax and Abbvie and has consulted for Incyte, Janssen, Morphosys and Novartis. He has received honoraria from Astra Zeneca and Kura for invited lectures and from Gilead for grant reviews. M.R. is on the scientific advisory board in Auron Pharmaceutical for which he received equity support. He receives research funding from Celularity, Roche-Genentech, Beat AML and NGM and travel fund from BD Biosciences. J.L.G. received consulting fees from GLG.W.X. has received research support from Stemline Therapeutics. P.G. has received research support from Paige.AI. M.B.G. has received research support from Sanofi, Amgen, and Actinium Pharmaceuticals, Inc., and has consulted for Novartis and Sanofi.
Figures




Comment in
-
Mixed-phenotype acute leukemia revisited: omics lead the way.Blood. 2025 May 1;145(18):1969-1971. doi: 10.1182/blood.2025028351. Blood. 2025. PMID: 40310658 No abstract available.
References
-
- Haematolymphoid Tumours. WHO Classification of Tumours. 5th edn, Vol. 11 (2024).
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
