

Early versus late nephrology referral and patient outcomes in chronic kidney disease: an updated systematic review and meta-analysis
- PMID: 39815172
- PMCID: PMC11737272
- DOI: 10.1186/s12882-025-03944-4
Early versus late nephrology referral and patient outcomes in chronic kidney disease: an updated systematic review and meta-analysis
Abstract
Background: Nephrology referral has been recognized as a modifiable factor influencing patient outcomes. The study aimed to compare clinical outcomes among patients referred early versus late to nephrologists.
Methods: We searched online database from inception to June 1, 2022, to obtain all eligible literature reporting outcomes of patients referred early versus late to nephrologists. The early and late referral was defined by the time at which patients were referred to nephrologists before dialysis onset.
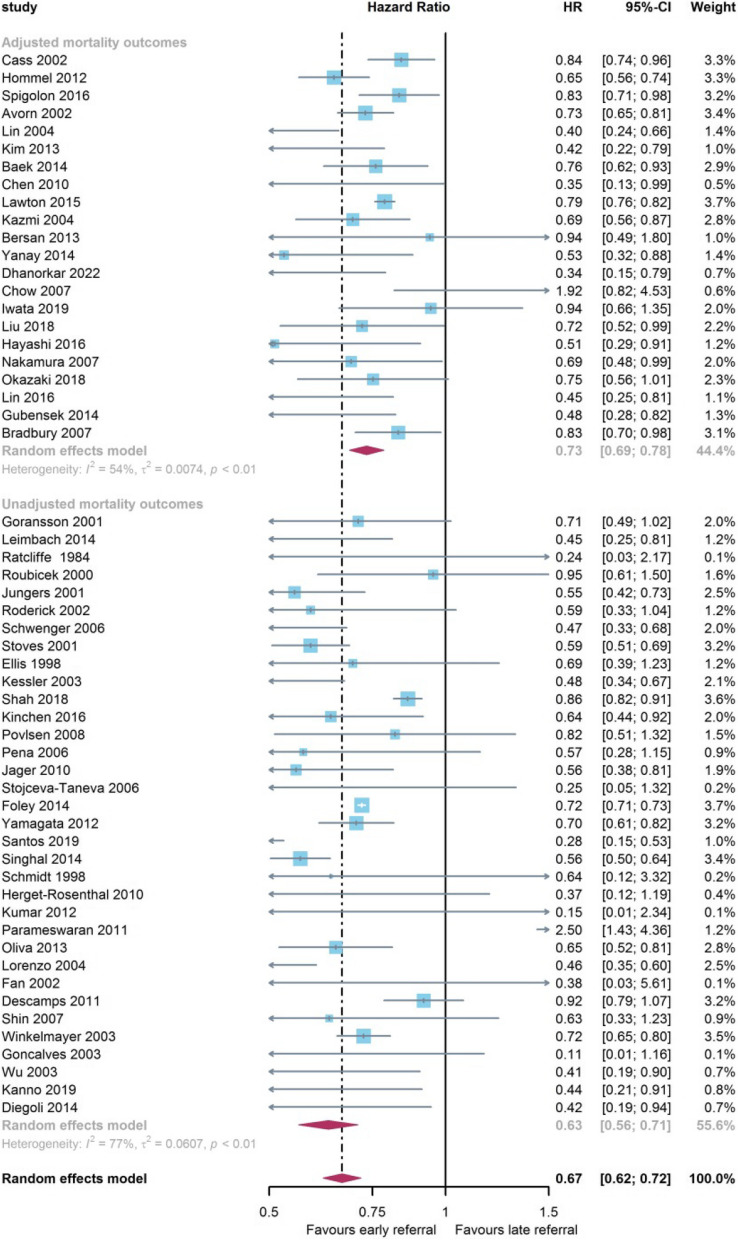
Results: Seventy-two studies with over 630,000 patients met the inclusion criteria. A lower likelihood of all-cause mortality (HR = 0.67, 95% CI: 0.62-0.72) was achieved among patients referred early to nephrologists. The survival advantage of early referral was apparent in the first 6 months and extended to the 5th year after dialysis onset (6 months: HR = 0.52, 95% CI: 0.40-0.68; 5 years: HR = 0.67, 95% CI: 0.60-0.74). The early referral was associated with shorter durations of initial hospitalization, a higher rate of kidney transplantation (RR = 1.41, 95% CI: 1.12-1.78), a lower likelihood of emergency start (RR = 0.39, 95% CI: 0.28-0.54), a higher likelihood of permanent access creation (RR = 3.34, 95% CI: 2.43-4.59), increased initial use of permanent access (RR = 2.60, 95% CI: 2.18-3.11), and reduced initial catheter use (RR = 0.43, 95% CI: 0.32-0.58).
Conclusions: Our study showed a lower risk of mortality, shorter lengths of initial hospitalization, and better preparations for renal replacement therapy among patients referred early to nephrologists. Early nephrology care should be promoted to improve the management of advanced chronic kidney disease.
Keywords: Chronic renal insufficiency; Meta-analysis; Mortality; Referral.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: An ethics statement is not applicable because this study is based exclusively on the published literature. The consent is not required because the study does not retrieve individual patients’ data. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures





Similar articles
-
Effect of early nephrology referral on the mortality of dialysis patients in Israel.Isr Med Assoc J. 2014 Aug;16(8):479-82. Isr Med Assoc J. 2014. PMID: 25269337
-
Factors Affecting the Referral Time to Nephrologists in Patients With Chronic Kidney Disease: A Prospective Cohort Study in Korea.Medicine (Baltimore). 2016 May;95(19):e3648. doi: 10.1097/MD.0000000000003648. Medicine (Baltimore). 2016. PMID: 27175688 Free PMC article.
-
The importance of early referral for the treatment of chronic kidney disease: a Danish nationwide cohort study.BMC Nephrol. 2012 Sep 10;13:108. doi: 10.1186/1471-2369-13-108. BMC Nephrol. 2012. PMID: 22963236 Free PMC article.
-
Primary and specialist care interaction and referral patterns for individuals with chronic kidney disease: a narrative review.BMC Nephrol. 2024 Apr 30;25(1):149. doi: 10.1186/s12882-024-03585-z. BMC Nephrol. 2024. PMID: 38689219 Free PMC article. Review.
-
Consequences of late referral on patient outcomes.Nephrol Dial Transplant. 2000;15 Suppl 3:8-13. doi: 10.1093/oxfordjournals.ndt.a027977. Nephrol Dial Transplant. 2000. PMID: 11032351 Review.
Cited by
-
Chronic kidney disease in the primary care setting: A narrative review.J Gen Fam Med. 2025 Jul 29;26(5):385-393. doi: 10.1002/jgf2.70054. eCollection 2025 Sep. J Gen Fam Med. 2025. PMID: 40904443 Free PMC article. Review.
-
Management and treatment of chronic kidney disease in the Danish Lolland-Falster Health Study: focus on renoprotection and cardiovascular disease prevention.Clin Kidney J. 2025 Aug 1;18(9):sfaf242. doi: 10.1093/ckj/sfaf242. eCollection 2025 Sep. Clin Kidney J. 2025. PMID: 40900939 Free PMC article.
References
-
- Liyanage T, Ninomiya T, Jha V, et al. Worldwide access to treatment for end-stage kidney disease: a systematic review. Lancet (London, England). 2015;385(9981):1975–82. - PubMed
-
- Kalantar-Zadeh K, Jafar TH, Nitsch D, et al. Chronic kidney disease. Lancet (London, England). 2021;398(10302):786–802. - PubMed
-
- Chan MR, Dall AT, Fletcher KE, et al. Outcomes in patients with chronic kidney disease referred late to nephrologists: a meta-analysis. Am J Med. 2007;120(12):1063–70. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
