

Delirium at the intensive care unit and long-term survival: a retrospective study
- PMID: 39815210
- PMCID: PMC11734231
- DOI: 10.1186/s12883-025-04025-7
Delirium at the intensive care unit and long-term survival: a retrospective study
Abstract
Background: Delirium is a common complication in patients at the intensive care unit (ICU) and is associated with prolonged ICU-stay and hospitalization and with increased morbidity. The impact of ICU-delirium on long-term survival is not clearly understood.
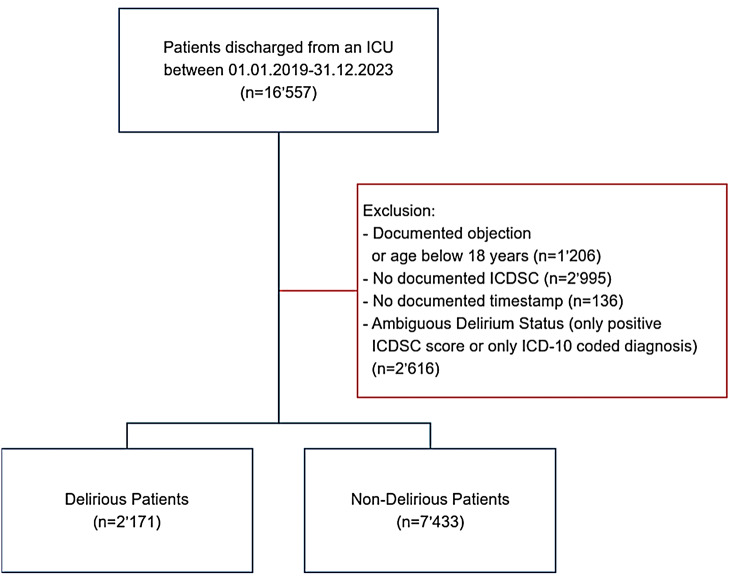
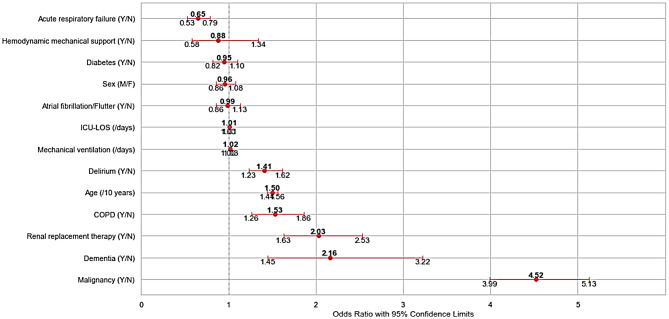
Methods: This retrospective single center observational study was conducted at the Institute of Intensive Care Medicine at the University Hospital Zurich, Switzerland. All adult ICU-survivors over a four-year period were screened for eligibility. ICU-delirium was defined based on the Intensive Care Delirium Screening Checklist (ICDSC), together with the coded diagnosis F05 in the International Classification of Diseases (ICD-2019). ICU-survivors who developed delirium during their ICU stay (group D) were compared with ICU-survivors who did not (group ND). Survival was evaluated according to data from hospital electronic health records up to four years from ICU-discharge. The survival analysis was reported using Kaplan-Meier curves and absolute risk differences (ARD). A multivariable logistic regression model was fitted with long-term survival at four years after ICU-discharge as outcome of interest, including several clinical conditions and interventions associated with long-term survival for ICU patients. For subgroup analysis, ICU-survivors were grouped based on age at the time of admission (45-54, 55-64, ≥ 65 years), and on relevant clinical conditions.
Results: A total of 9'604 patients fulfilled the inclusion criteria, of them 22.6% (n = 2'171) developed ICU-delirium. Overall, patients in the group D had a significantly lower probability of survival than patients in the group ND (p < 0.0001, ARD = 11.8%). In the multivariable analysis, ICU-delirium was confirmed as independently associated with long-term survival. After grouping for age categories, patients between 55 and 64 years of age in the group D were less likely to survive than patients in the group ND at every time point analyzed, up to four years after ICU discharge (p < 0.001, ARD = 7.3%). This difference was even more significant in the comparison between patients over 65 years (p < 0.0001, ARD 11.1%). No significant difference was observed in the other age groups.
Conclusions: In the study population, ICU-delirium was independently associated with a reduced long-term survival. Patients who developed ICU-delirium had a reduced survival up to four years after ICU discharge and this association was particularly evident in patients above 55 years of age.
Keywords: Delirium; Encephalopathy; ICU; Long-term survival.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the cantonal ethics committee of Zurich (BASEC: 2020–02695). The study complies with the Declaration of Helsinki, the Guidelines on Good Clinical Practice (GCP-Directive) issued by the European Medicines Agency as well as with Swiss law and regulatory authority requirements. Consent for publication: Informed consent was obtained from the patients or from their relatives whenever possible. The cantonal ethics committee of Zurich granted permission to use the data of all patients who did not object to the use of their data for research purposes. Competing interests: The authors declare no competing interests.
Figures

Similar articles
-
Delirium and Weakness Acquired in the Intensive Care Unit: Individual and Combined Effects on 90-Day Mortality in Survivors of Critical Illness.J Clin Nurs. 2025 Sep;34(9):3620-3627. doi: 10.1111/jocn.17517. Epub 2024 Oct 29. J Clin Nurs. 2025. PMID: 39468861
-
Assessing the Risk of Delirium and Death in Sepsis Using the Braden Score: A Retrospective Study.J Clin Nurs. 2025 Jul;34(7):2779-2790. doi: 10.1111/jocn.17476. Epub 2024 Oct 11. J Clin Nurs. 2025. PMID: 39394637
-
[Association of serum potassium trajectory with 30-day death risk in patients with sepsis in intensive care unit: a retrospective cohort study].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2025 Apr;37(4):324-330. doi: 10.3760/cma.j.cn121430-20240726-00635. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2025. PMID: 40814703 Chinese.
-
The confusion assessment method for the intensive care unit (CAM-ICU) and intensive care delirium screening checklist (ICDSC) for the diagnosis of delirium: a systematic review and meta-analysis of clinical studies.Crit Care. 2012 Jul 3;16(4):R115. doi: 10.1186/cc11407. Crit Care. 2012. PMID: 22759376 Free PMC article.
-
Diagnostic accuracy of the pediatric CAM-ICU, pre-school CAM-ICU, Pediatric Anesthesia Emergence Delirium and Cornell Assessment of Pediatric Delirium for detecting delirium in the pediatric intensive care unit: A systematic review and meta-analysis.Intensive Crit Care Nurs. 2024 Jun;82:103606. doi: 10.1016/j.iccn.2023.103606. Epub 2023 Dec 29. Intensive Crit Care Nurs. 2024. PMID: 38158251
References
-
- Ouimet S, Riker R, Bergeron N, Cossette M, Kavanagh B, Skrobik Y. Subsyndromal delirium in the ICU: evidence for a disease spectrum. Intensive Care Med. 2007;33(6):1007–13. - PubMed
-
- van den Boogaard M, Schoonhoven L, van der Hoeven JG, van Achterberg T, Pickkers P. Incidence and short-term consequences of delirium in critically ill patients: a prospective observational cohort study. Int J Nurs Stud. 2012;49(7):775–83. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
