

Clinical and imaging features of co-existent pulmonary tuberculosis and lung cancer: a population-based matching study in China
- PMID: 39815214
- PMCID: PMC11734471
- DOI: 10.1186/s12885-024-13350-y
Clinical and imaging features of co-existent pulmonary tuberculosis and lung cancer: a population-based matching study in China
Abstract
Background: Co-existent pulmonary tuberculosis and lung cancer (PTB-LC) represent a unique disease entity often characterized by missed or delayed diagnosis. This study aimed to investigate the clinical and radiological features of patients diagnosed with PTB-LC.
Methods: Patients diagnosed with active PTB-LC (APTB-LC), inactive PTB-LC (IAPTB), and LC alone without PTB between 2010 and 2022 at our institute were retrospectively collected and 1:1:1 matched based on gender, age, and time of admission. Symptoms and clinicopathological features were compared among the three groups of patients. Logistic regression was employed for risk factor analysis.
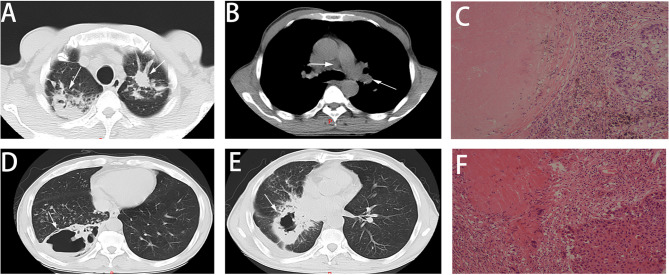
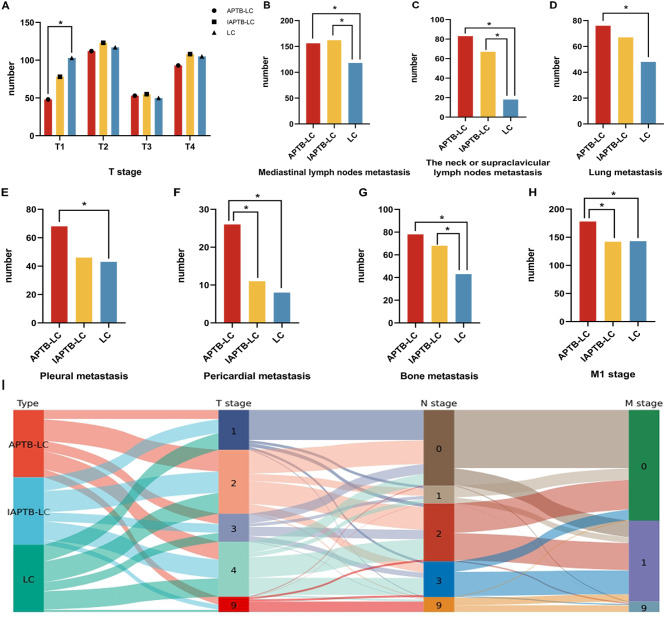
Results: Compared to LC or IAPTB-LC, patients with APTB-LC exhibited higher proportions of weight loss (p < 0.001) and fever (p < 0.001) at the time of diagnosis. Additionally, radiological features such as nodules (p = 0.007), tree-in-bud (p < 0.001), cavitation (p < 0.001), and calcification (p < 0.001) were significantly more prevalent in APTB-LC patients compared to the other groups. Patients with APTB-LC were more susceptible to lymph node involvement (p < 0.001) and distant metastasis (p = 0.006) compared to those with IAPTB-LC or LC alone. Additionally, in comparison to LC alone, patients with IAPTB-LC exhibited more complex symptoms, imaging features, and lymph node metastases. Logistic regression results indicated that factors such as BMI, fever, patchy shadow, cavitation, neck or supraclavicular lymph node metastasis, and liver injury favor the diagnosis of APTB-LC over LC alone. The pre-diagnostic model exhibited robust performance, achieving area under the curve (AUC) values of 0.864 in the training set and 0.830 in the test set.
Conclusion: Our results indicate that PTB-LC is a distinct disease characterized by complex clinicopathological features and a more aggressive nature. Based on our findings, we recommend conducting TB-related tests for LC patients who exhibit relevant risk factors or are identified as high-risk cases according to the pre-diagnostic model.
Keywords: CT imaging; Clinical features; Lung cancer; TNM stage; Tuberculosis.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by the Ethics Committee of Beijing Chest Hospital (ID, JS-2023-10). This project was deemed exempt from the requirement for informed consent, which was approved by Ethics Committee of Beijing Chest Hospital. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

Similar articles
-
Use of low-dose computed tomography to assess pulmonary tuberculosis among healthcare workers in a tuberculosis hospital.Infect Dis Poverty. 2017 Mar 24;6(1):68. doi: 10.1186/s40249-017-0274-6. Infect Dis Poverty. 2017. PMID: 28335802 Free PMC article.
-
Associated factors of co-existent pulmonary tuberculosis and lung cancer: A case-control study.Eur J Clin Invest. 2021 Apr;51(4):e13432. doi: 10.1111/eci.13432. Epub 2020 Nov 10. Eur J Clin Invest. 2021. PMID: 33053200
-
Evaluation of the diagnostic efficacy of 18 F-Fluorine-2-Deoxy-D-Glucose PET/CT for lung cancer and pulmonary tuberculosis in a Tuberculosis-endemic Country.Cancer Med. 2020 Feb;9(3):931-942. doi: 10.1002/cam4.2770. Epub 2019 Dec 13. Cancer Med. 2020. PMID: 31837121 Free PMC article.
-
Misdiagnosis of a multi-organ involvement hematogenous disseminated tuberculosis as metastasis: a case report and literature review.Infect Dis Poverty. 2020 Jun 9;9(1):66. doi: 10.1186/s40249-020-00681-8. Infect Dis Poverty. 2020. PMID: 32517798 Free PMC article. Review.
-
Imaging modalities for pulmonary tuberculosis in children: A systematic review.Eur J Radiol Open. 2022 Dec 30;10:100472. doi: 10.1016/j.ejro.2022.100472. eCollection 2023. Eur J Radiol Open. 2022. PMID: 36624819 Free PMC article. Review.
Cited by
-
Establishment and validation of a convenient and efficient screening tool for active pulmonary tuberculosis in lung cancer patients based on common parameters.Ther Adv Med Oncol. 2025 Jul 24;17:17588359251355058. doi: 10.1177/17588359251355058. eCollection 2025. Ther Adv Med Oncol. 2025. PMID: 40727884 Free PMC article.
References
-
- World Health Organization. Global tuberculosis report 2023. [ https://www.who.int/publications/i/item/9789240083851
-
- Leiter A, Veluswamy RR, Wisnivesky JP. The global burden of lung cancer: current status and future trends. Nat Rev Clin Oncol. 2023;20(9):624–39. - PubMed
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global Cancer statistics 2020: GLOBOCAN estimates of incidence and Mortality Worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–49. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
