

Role of bilevel erector spinae with high thoracic block vs conventional unilevel block in analgesia and reduction of pain in axilla in breast cancer surgeries: a randomized controlled trial
- PMID: 39816904
- PMCID: PMC11732649
- DOI: 10.1097/PR9.0000000000001234
Role of bilevel erector spinae with high thoracic block vs conventional unilevel block in analgesia and reduction of pain in axilla in breast cancer surgeries: a randomized controlled trial
Abstract
Introduction: Management of pain associated with breast cancer surgeries is crucial in reducing incidence of postmastectomy pain syndrome. The pain distribution involves the anterior chest wall, axillary area and ipsilateral upper limb.
Objective: This study was designed to investigate the effect of bilevel erector spinae plane block (ESPB) with high thoracic block vs the conventional unilevel ESPB vs opioids in patients with cancer undergoing modified radical mastectomy regarding pain control and reducing pain in axilla.
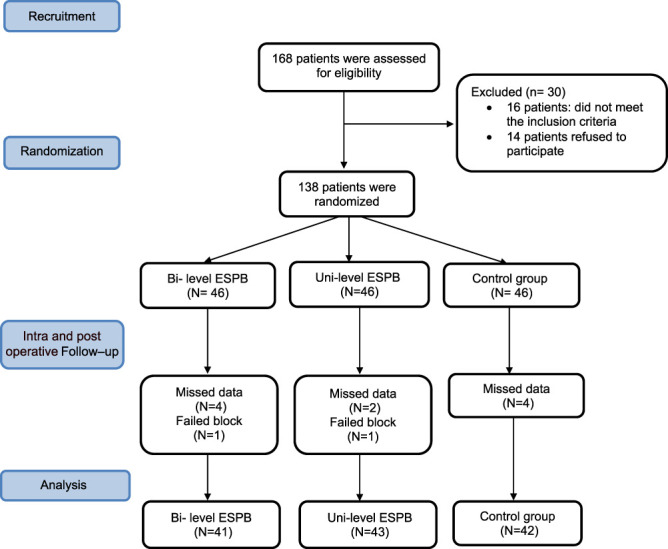
Methods: One hundred twenty-six female patients with cancer and American Society of Anesthesiology II, III were randomized into 3 groups: bilevel ESPB, unilevel ESPB, and control group. The primary outcome was total postoperative morphine consumption.
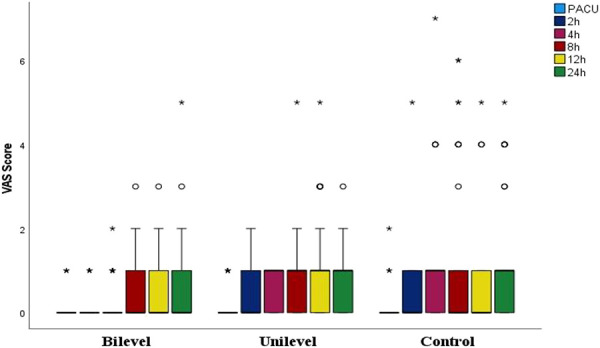
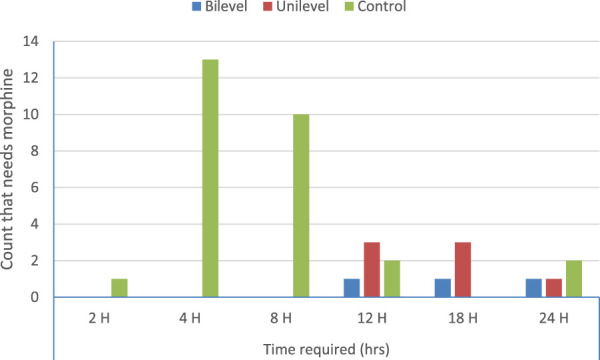
Results: Total postoperative morphine consumption was higher for the control group compared with the bilevel and unilevel groups (5.5 ± 1.8 vs 3.0 ± 0.0 and 4.3 ± 1.6 mg, P = 0.038). First time to receive morphine was longer for bilevel and unilevel groups compared with the control group (20.7 ± 3.1 and 17.7 ± 4.1 vs 8.2 ± 5 hours, P < 0.001). There was 96.1% and 90.3% reduction in morphine intake with odds ratio 25.6 (95% confidence interval [CI]: 6.6-100) and 10.3 (95% CI: 3.7-28.6) for the bilevel and unilevel groups compared with the control group. There was 98.5% and 65.4% reduction in the incidence of pain in axilla with odds ratio 66.6 (95% CI: 16.9-250) and 21.7 (95% CI: 6.75-66.6) for the bilevel and unilevel groups compared with the control group. Postoperative visual analog scale was lower for the bilevel group after 2, 4, and 24 hours compared with both the control group and the unilevel groups, P < 0.005.
Conclusion: Both conventional unilevel and high thoracic bilevel ESPB had better analgesic profile when compared with opioids. Although the bilevel ESPB had additional merits to the unilevel ESPB in analgesic effects, both can be used effectively.
Keywords: Analgesia; Breast; Cancer; ESPB; Morphine; Pain.
Copyright © 2025 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of The International Association for the Study of Pain.
Conflict of interest statement
The authors have no conflicts of interest to declare. Data availability: data generated will be available for 1 year through contacting the corresponding author upon reasonable request. Institutional Review Board number: 2205-501-007. Clinical trial registration: NCT05429489.Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures
References
-
- Aksu C, Kuş A, Yörükoğlu HU, Tor Kiliç C, Gürkan Y. Analgesic effect of the bi-level injection erector spinae plane block after breast surgery: a randomized controlled trial. Agri 2019;31:132–7. - PubMed
-
- Capuco A, Urits I, Orhurhu V, Chun R, Shukla B, Burke M, Kaye RJ, Garcia AJ, Kaye AD, Viswanath O. A comprehensive review of the diagnosis, treatment, and management of postmastectomy pain syndrome. Curr Pain Headache Rep 2020;24:41. - PubMed
LinkOut - more resources
Full Text Sources
Medical