

The efficacy and safety of intrinsic antitachycardia pacing
- PMID: 39817024
- PMCID: PMC11730729
- DOI: 10.1002/joa3.13221
The efficacy and safety of intrinsic antitachycardia pacing
Abstract
Background: The clinical outcomes of a novel antitachycardia pacing (ATP) algorithm-intrinsic ATP (iATP)-compared to conventional ATP (cATP) have yet to be fully elucidated.
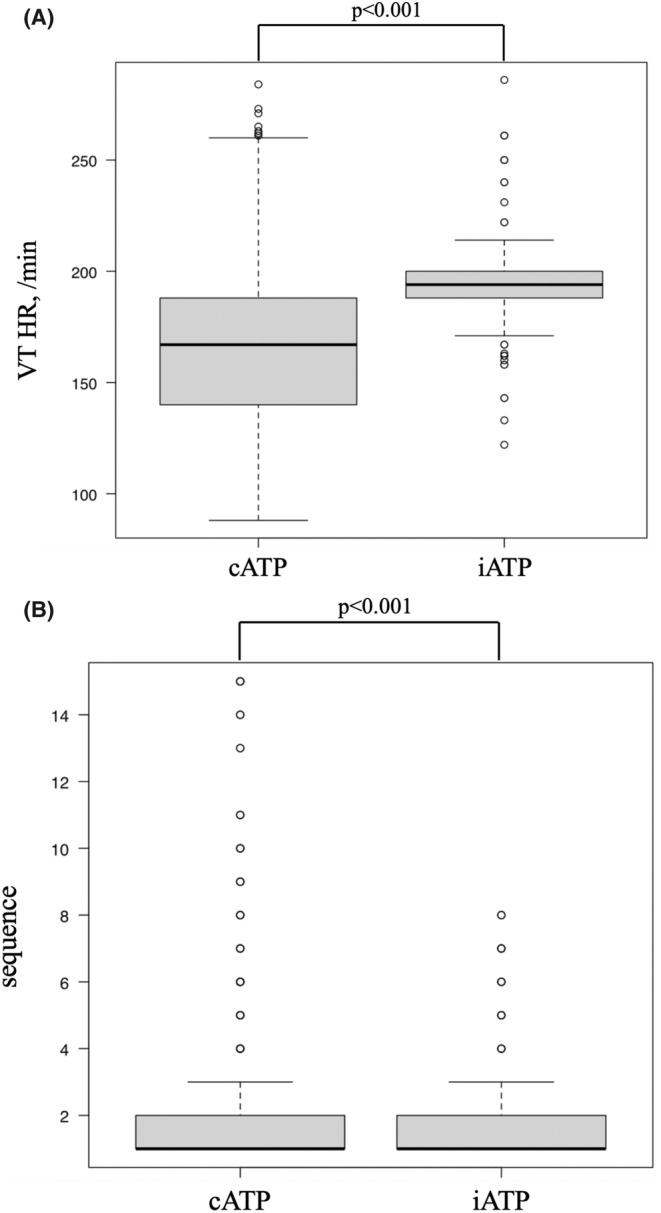
Methods: This retrospective study analyzed 128 patients and 1962 ventricular tachycardia (VT) episodes treated with the iATP or the cATP at Kokura Memorial Hospital. Patients were categorized into two groups: the iATP group (23 patients, 182 episodes) and the cATP group (105 patients, 1780 episodes). We evaluated ATP success rates and baseline patient characteristics on a per-patient basis. Additionally, we extracted VT that were not terminated by a single ATP and compared ATP success rates using propensity score matching.
Results: Per patient; The iATP group exhibited significantly lower creatinine levels (1.18 ± 0.40 mg/dL vs. 1.82 ± 1.61 mg/dL, p = .021) and a shorter follow-up period (609 ± 323 days vs. 1017 ± 252 days, p < .001) compared to the cATP group. ATP success was observed in 19 patients in the iATP group and 62 patients in the cATP group (82.6% vs. 59%, p = .054). Per episode; there was no significant difference in ATP success rate (91.8% vs. 92.7%, p = .645) or in acceleration rate (1.1% vs. 2.4%, p = .274). However, when limited to episodes in which VT was not terminated by a single ATP and propensity score matching was performed, the iATP showed a higher VT termination rate (84.1% vs. 53.6%, p < .001) and a lower acceleration rate (0% vs. 10.1%, p = .013) than the cATP.
Conclusions: The efficacy and safety of the iATP for VT that was not terminated by the first sequence of ATP was demonstrated.
Keywords: acceleration; implantable cardioverter defibrillator; intrinsic antitachycardia pacing; postpacing interval; ventricular tachycardia.
© 2025 The Author(s). Journal of Arrhythmia published by John Wiley & Sons Australia, Ltd on behalf of Japanese Heart Rhythm Society.
Conflict of interest statement
All authors have no relevant financial or nonfinancial interests to disclose.
Figures


References
-
- Piccini JP, Al‐Khatib SM, Hellkamp AS, Anstorm KA, Poole JE, Mark DE, et al. Mortality benefits from implantable cardioverter‐ defibrillator therapy are not restricted to patients with remote myocardial infarction: an analysis from the sudden cardiac death in heart failure trial (SCD‐HeFT). Heart Rhythm. 2011;8:393–400. - PMC - PubMed
-
- Sweeney M, Sherfesee L, DeGroot PJ, Wathen M, Wilkoff B. Differences in effects of electrical therapy type for ventricular arrhythmias on mortality in implantable cardioverter‐defibrillator patients. Heart Rhythm. 2010;7:353–360. - PubMed
-
- Swenson DJ, Taepke RT, Blauer JJE, Kwan E, Ghafoori E, Plank G, et al. Direct comparison of a novel antitachycardia pacing algorithm against present methods using virtual patient modeling. Heart Rhythm. 2020;17:1602–1608. - PubMed
-
- Kamakura T, Ueda N, Wada M, Ishibashi K, Kusano K. Efficacy of intrinsic antitachycardia pacing for ventricular tachycardia refractory to conventional burst pacing: a case series. J Cardiovasc Electrophysiol. 2023;34:225–228. - PubMed
LinkOut - more resources
Full Text Sources
