

Association of preoperative blood biomarkers with postoperative major adverse cardiac events and mortality in major orthopaedic surgery: a systematic review and meta-analysis
- PMID: 39819956
- PMCID: PMC11752069
- DOI: 10.1136/bmjopen-2024-086263
Association of preoperative blood biomarkers with postoperative major adverse cardiac events and mortality in major orthopaedic surgery: a systematic review and meta-analysis
Abstract
Objective: The association between preoperative blood biomarkers and major adverse cardiac events (MACEs) as well as mortality after major orthopaedic surgery remains unclear. This study aimed to assess the association between preoperative blood biomarkers and postoperative MACEs as well as all-cause mortality in patients undergoing major orthopaedic surgery.
Design: A systematic review and meta-analysis.
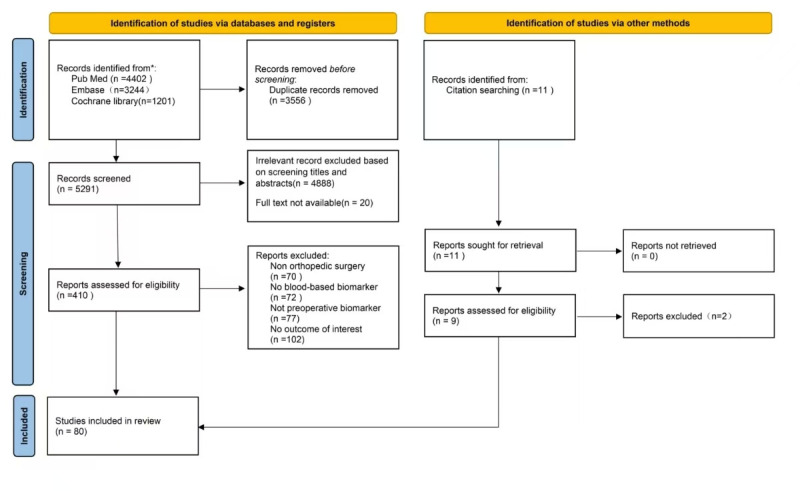
Data sources: PubMed, EMBASE, the Cochrane Controlled Trials Register and Cochrane Database of Systematic Reviews from inception to 20 October 2024 were searched.
Eligibility criteria: Observational or experimental studies reporting the correlation between preoperative blood biomarkers and postoperative MACEs-categorised as short-term (within 3 months) or long-term (beyond 3 months)-and all-cause mortality in patients undergoing major orthopaedic surgery.
Data extraction and synthesis: Data from studies reporting OR or HR and its 95% CI were pooled for analysis using random-effects model.
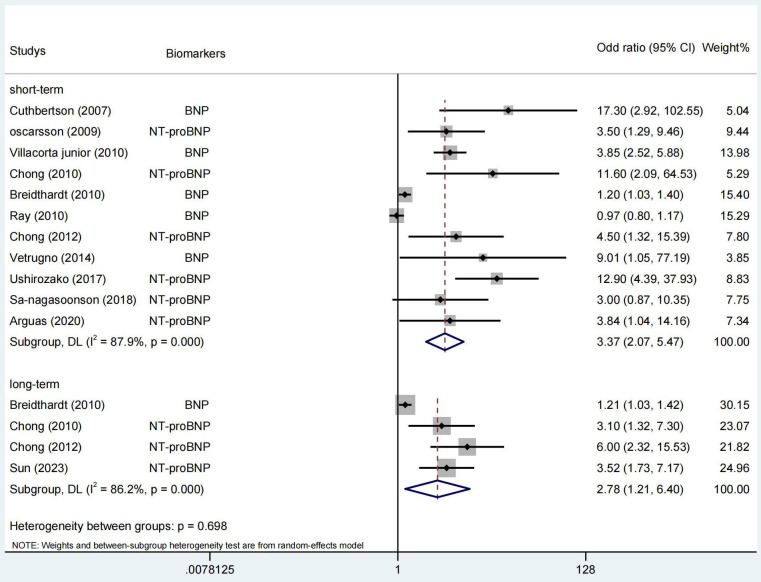
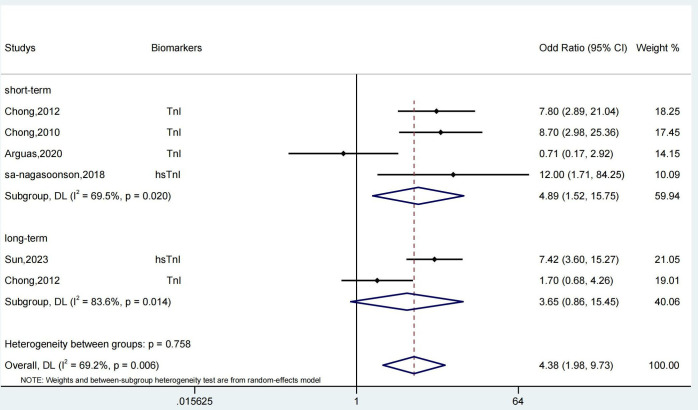
Results: 21 preoperative blood-based biomarkers from 80 studies with 226 468 patients were analysed. Elevated preoperative cardiac biomarkers were correlated with a heightened risk of MACEs within 3 months (natriuretic peptide: OR 3.37, 95% CI 2.07 to 5.47, I2=87.9%; cardiac troponin: OR 4.89, 95% CI 1.52 to 15.75, I2=69.5%) with significant heterogeneity. Only natriuretic peptide was associated with a high-risk long-term MACEs (>3 months) (OR 3.52, 95% CI 1.73 to 7.17, I2=86.2%). In contrast, cardiac biomarkers were not identified as having prognostic value for all-cause mortality in this patient cohort. Additionally, an increased risk of all-cause mortality was associated with preoperative abnormal levels of albumin (OR 1.15, 95% CI 1.06 to 1.24, I2=84.8%), creatinine (OR 1.54, 95% CI 1.12 to 1.95, I2=0), 25(OH)D (OR 1.58, 95% CI 1.01 to 2.14, I2=0) and glomerular filtration rate (GFR) (OR 1.12, 95% CI 1.06 to 1.17, I2=0), rather than cardiac biomarkers.
Conclusions: The study proposed that cardiac biomarkers assessed before surgery could offer prognostic insight into short-term MACEs, while preoperative abnormal levels of albumin, creatinine, 25 (OH)D and GFR might be prognostic valuable for all-cause mortality following major orthopaedic surgery.
Prospero registration number: CRD42022352091.
Keywords: Anaesthesia in orthopaedics; Meta-Analysis; Mortality.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Association of pre-operative troponin levels with major adverse cardiac events and mortality after noncardiac surgery: A systematic review and meta-analysis.Eur J Anaesthesiol. 2018 Nov;35(11):815-824. doi: 10.1097/EJA.0000000000000868. Eur J Anaesthesiol. 2018. PMID: 30095548
-
Systematic review and meta-analysis of postoperative troponin as a predictor of mortality and major adverse cardiac events after vascular surgery.J Vasc Surg. 2020 Sep;72(3):1132-1143.e1. doi: 10.1016/j.jvs.2020.03.039. Epub 2020 Apr 17. J Vasc Surg. 2020. PMID: 32305383
-
Prognostic performance of preoperative cardiac troponin and perioperative changes in cardiac troponin for the prediction of major adverse cardiac events and mortality in noncardiac surgery: A systematic review and meta-analysis.PLoS One. 2019 Apr 22;14(4):e0215094. doi: 10.1371/journal.pone.0215094. eCollection 2019. PLoS One. 2019. PMID: 31009468 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Absolute Postoperative B-Type Natriuretic Peptide Concentrations, but Not Their General Trend, Are Associated With 12-Month, All-Cause Mortality After On-Pump Cardiac Surgery.Anesth Analg. 2017 Sep;125(3):753-761. doi: 10.1213/ANE.0000000000002291. Anesth Analg. 2017. PMID: 28753169
References
-
- Beckerly R, Avram MJ. Clinical Anesthesia Procedures of the Massachusetts General Hospital, Eighth Edition. Anesthesiology. 2011;115:663. doi: 10.1097/ALN.0b013e31821f8eb0. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical