

Resin composite aggregated S-PRG particles are not superior to non-S-PRG under microcosm biofilm
- PMID: 39820496
- PMCID: PMC11739560
- DOI: 10.1038/s41598-024-78396-1
Resin composite aggregated S-PRG particles are not superior to non-S-PRG under microcosm biofilm
Abstract
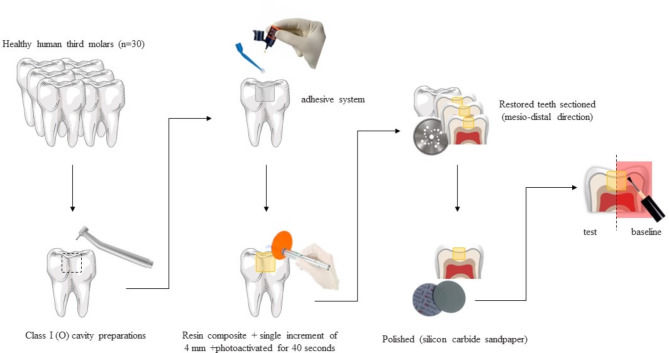
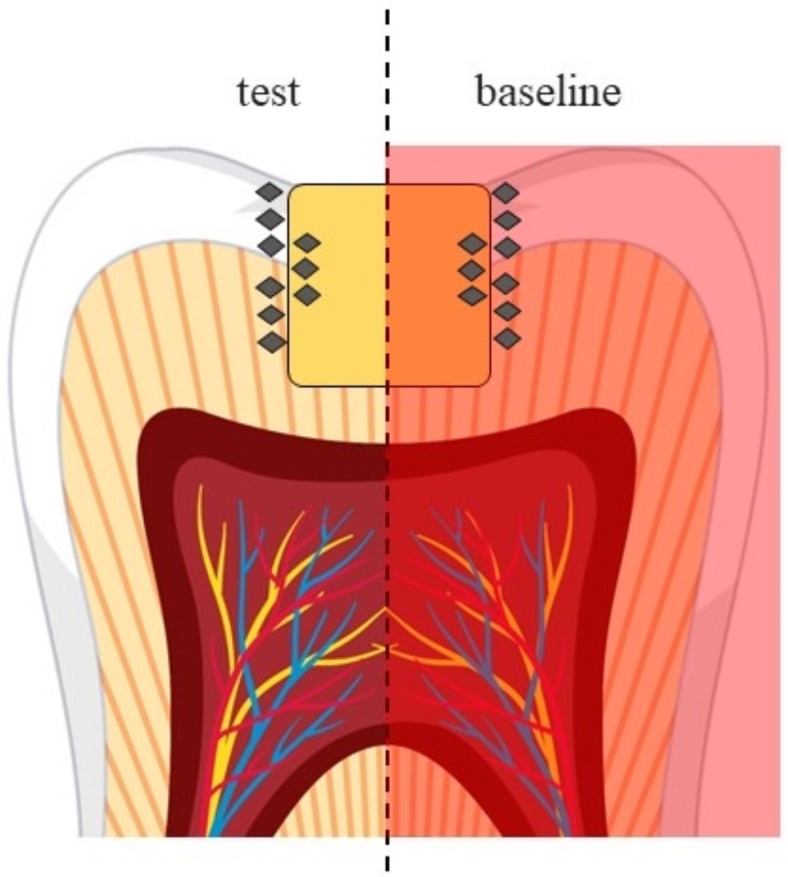
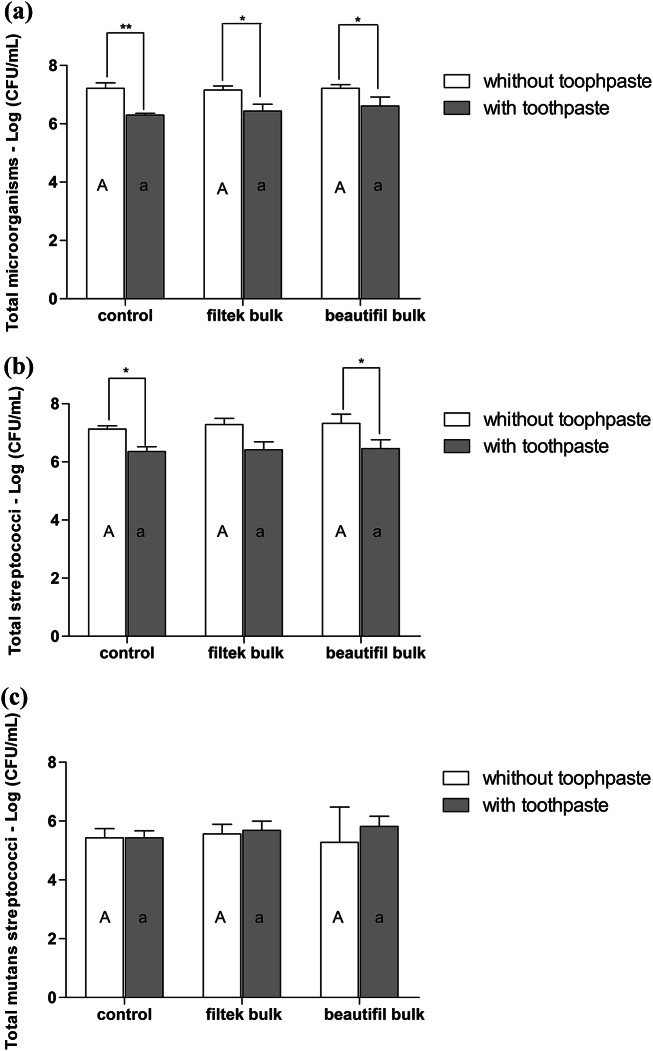
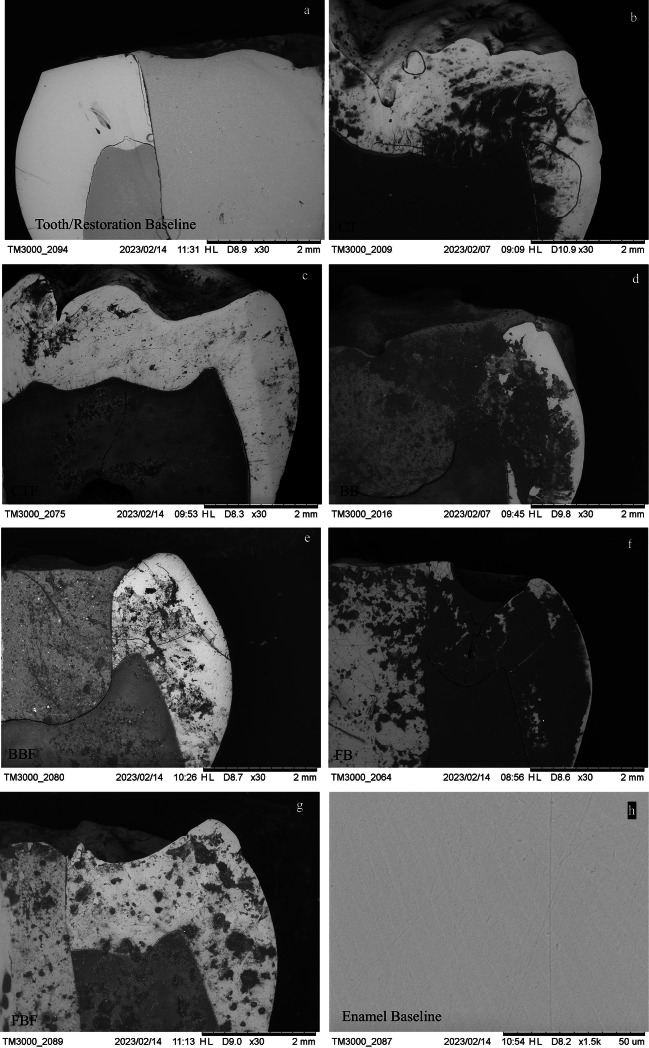
This study assessed the effect of composite resins, aggregated or not with S-PRG particles, and the use of toothpaste in controlling demineralization and bacterial growth. Human molars were distributed into 3 groups: control (CT) - sound teeth, Beautifil Bulk Restorative System (aggregated with S-PRG) (BB), Filtek One Bulk Fill (without S-PRG) (FB). Teeth destined for groups BB and FB previously received Class I preparations (4 × 4 × 4 mm), followed by single-increment restorations. All teeth were sectioned mesiodistally, with all specimens subjected to cariogenic challenge for 5 days, including microcosm biofilm formation. Half of each tooth was exposed to toothpaste (CTF, BBF, FBF). The loss of microhardness was assessed considering the initial microhardness as 100% on enamel, dentin, and composite resin substrates. Colony Forming Units (CFU/mL) were counted in 3 media. Data analysis used one-way ANOVA, Tukey HSD test, and paired t-test (α = 0.05). Toothpaste significantly reduced CFU/mL for total bacteria and genus Streptococcus (p < 0.05), with no significant difference for Streptococcus mutans. Enamel microhardness was positively affected by toothpaste. Both restorative systems controlled enamel demineralization, with FB and FBF outperforming BB and BBF. There was minor degradation of both composite resins, between 10% and 22%. Toothpaste effectively reduced microorganisms, irrespective of the composite resin. Regarding demineralization control, both restorative systems, with and without S-PRG particles, were effective on enamel.
Keywords: Demineralization; Dental caries; Resin composite; Secondary caries; Toothpaste.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethics approval: All procedures performed in this study involving human teeth were in accordance with the ethical standards of the institutional and national human research committee (CEP/UFMS - Federal University of Mato Grosso do Sul (MS/Brazil); protocol: 3.678.506, CAAE: 21527119.6.0000.0021) and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Informed consent: Informed consent was obtained from all individual participants included in the study.
Figures




References
-
- Eltahlah, D., Lynch, C. D., Chadwick, B. L., Blum, I. R. & Wilson N.H.F. An update on the reasons for placement and replacement of direct restorations. J. Dent.72 (5), 1–7. 10.1016/j.jdent.2018.03.001 (2018). - PubMed
-
- Aminoroaya, A. et al. A review of dental composites: challenges, chemistry aspects, filler influences, and future insights. Compos. Part. B. 216, 108852. 10.1016/j.compositesb.2021.108852 (2021).
-
- Demarco, F. F. et al. N.J.M. Longevity of composite restorations is definitely not only about materials. Dent. Mater.39 (1), 1–12. 10.1016/j.dental.2022.11.009 (2023). - PubMed
-
- Maran, B. M. et al. Nanofilled/nanohybrid and hybrid resin-based composite in patients with direct restorations in posterior teeth: a systematic review and meta-analysis. J. Dent.99 (8), 103407. 10.1016/j.jdent.2020.103407 (2020). - PubMed
-
- Veloso, S. R. M. et al. Clinical performance of bulk-fill and conventional resin composite restorations in posterior teeth: a systematic review and meta-analysis. Clin. Oral Investig. 23 (1), 221–233. 10.1007/s00784-018-2429-7 (2019). - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
