

Head and neck paraganglioma in Pacak-Zhuang syndrome
- PMID: 39821441
- PMCID: PMC11790058
- DOI: 10.1093/jncics/pkaf001
Head and neck paraganglioma in Pacak-Zhuang syndrome
Abstract
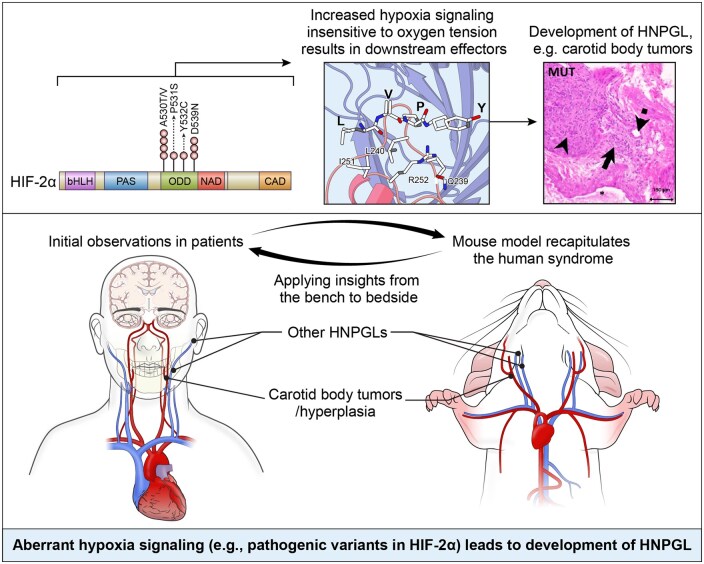
Background: Head and neck paragangliomas (HNPGLs) are typically slow-growing, hormonally inactive tumors of parasympathetic paraganglia. Inactivation of prolyl-hydroxylase domain-containing 2 protein causing indirect gain-of-function of hypoxia-inducible factor-2α (HIF-2α), encoded by EPAS1, was recently shown to cause carotid body hyperplasia. We previously described a syndrome with multiple sympathetic paragangliomas caused by direct gain-of-function variants in EPAS1 (Pacak-Zhuang syndrome, PZS) and developed a corresponding mouse model.
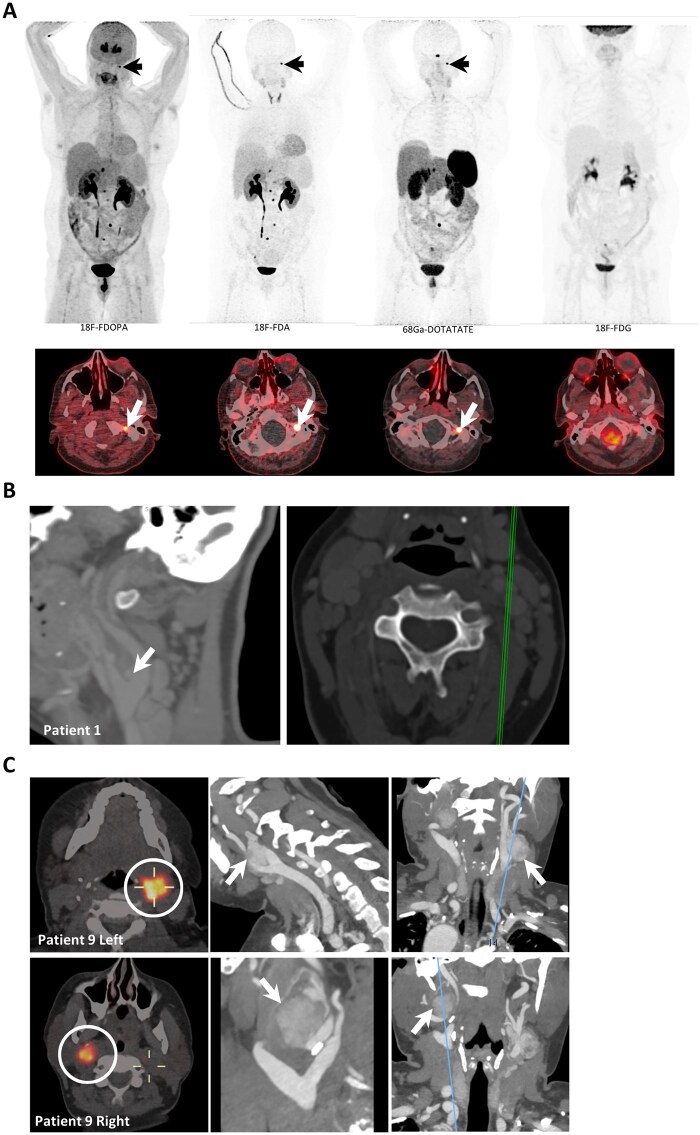
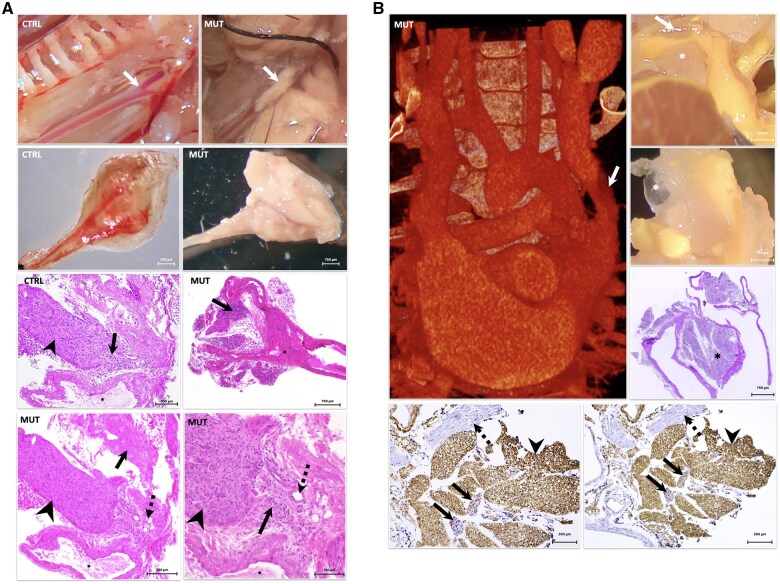
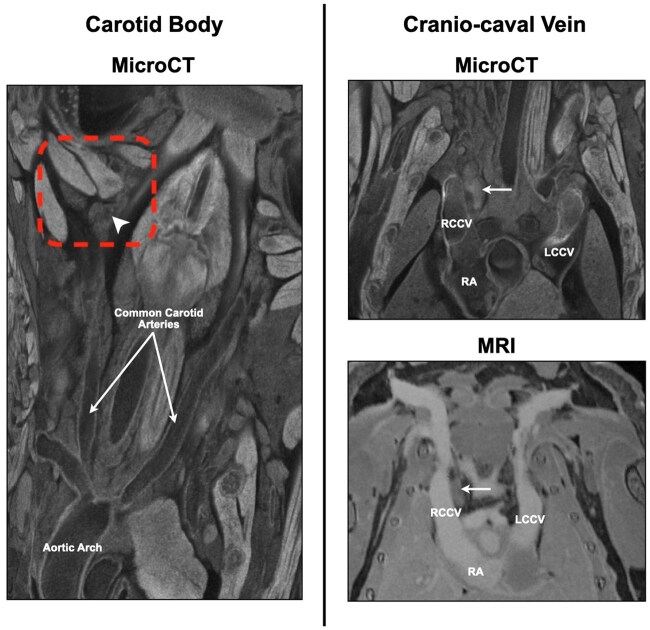
Methods: We evaluated a cohort of patients with PZS (n = 9) for HNPGL by positron emission tomography, magnetic resonance imaging, and computed tomography and measured carotid body size compared to literature reference values. Resected tumors were evaluated by histologic sectioning and staining. We evaluated the corresponding mouse model at multiple developmental stages (P8 and adult) for lesions of the head and neck by high resolution ex vivo imaging and performed immunohistochemical staining on histologic sections of the identified lesions.
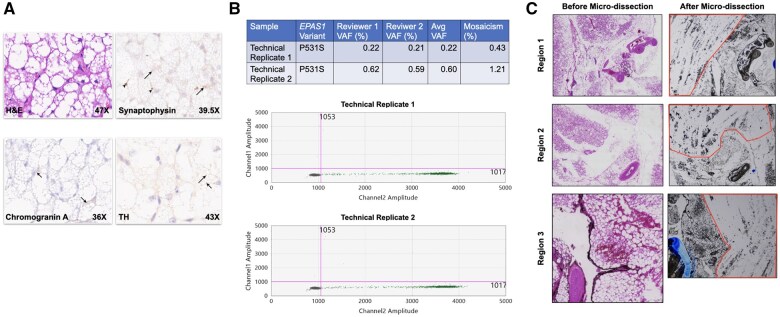
Results: hree patients had imaging consistent with HNPGL, one of which warranted resection and was confirmed on histology. Three additional patients had carotid body enlargement (Z-score > 2.0), and 3 had carotid artery malformations. We found that 9 of 10 adult variant mice had carotid body tumors and 6 of 8 had a paraganglioma on the cranio-caval vein, the murine homologue of the superior vena cava; these were also found in 4 of 5 variant mice at post-natal day 8. These tumors and the one resected from a patient were positive for tyrosine hydroxylase, synaptophysin, and chromogranin A. Brown fat in a resected patient tumor carried the EPAS1 pathogenic variant.
Conclusions: These findings (1) suggest HNPGL as a feature of PZS and (2) show that these pathogenic variants are sufficient to cause the development of these tumors, which we believe represents a continuous spectrum of disease starting from hyperplasia.
Published by Oxford University Press 2025.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials