

Enlightening the invisible: Applications, limits and perspectives of intraoperative fluorescence in neurosurgery
- PMID: 39823065
- PMCID: PMC11735926
- DOI: 10.1016/j.bas.2024.103928
Enlightening the invisible: Applications, limits and perspectives of intraoperative fluorescence in neurosurgery
Abstract
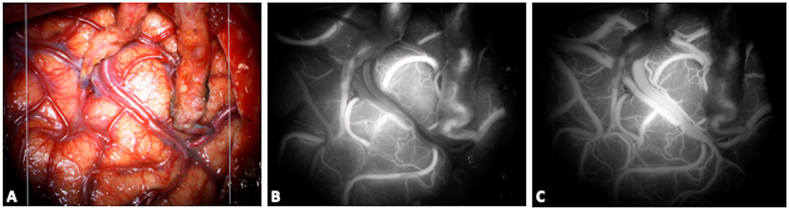
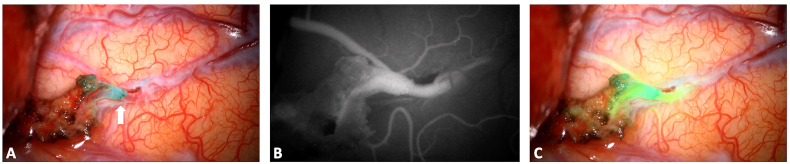
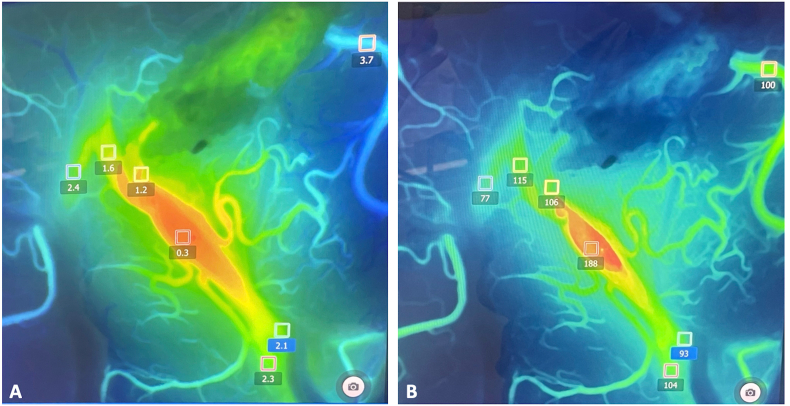
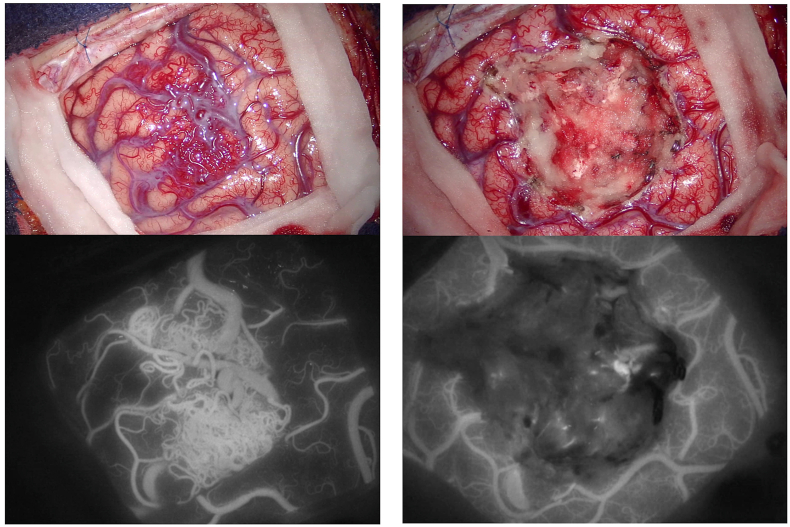
Introduction: The introduction of intraoperative fluorophores represented a significant advancement in neurosurgical practice. Nowadays they found different applications: in oncology to improve the visualization of tumoral tissue and optimize resection rates and in vascular neurosurgery to assess the exclusion of vascular malformations or the permeability of bypasses, with real-time intraoperative evaluations.
Research question: A comprehensive knowledge of how fluorophores work is crucial to maximize their benefits and to incorporate them into daily neurosurgical practice. We would like to revise here their applications and clinical relevance.
Material and methods: A focused literature review of relevant articles dealing with the versatile applications of fluorophores in neurosurgery was performed.
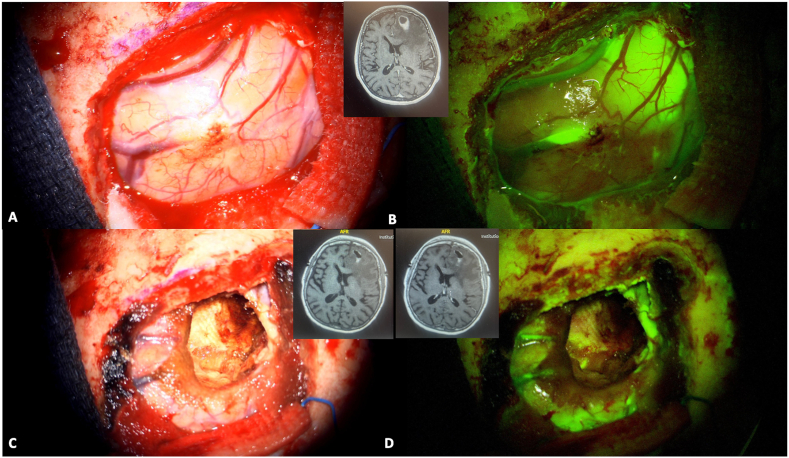
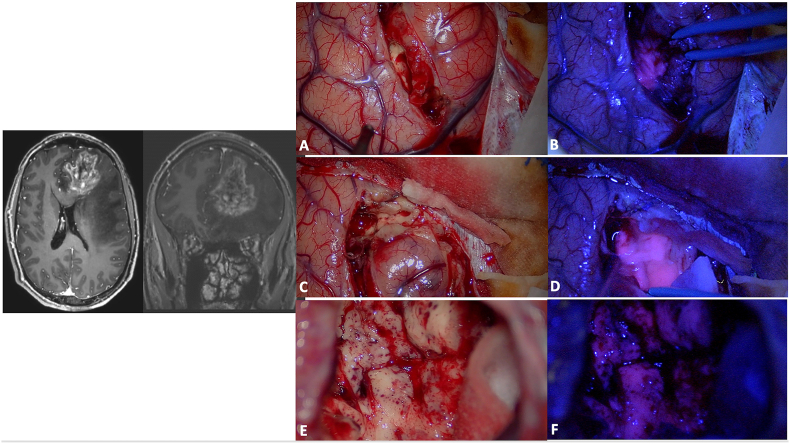
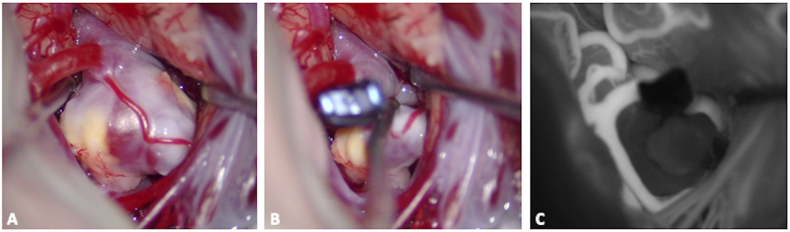
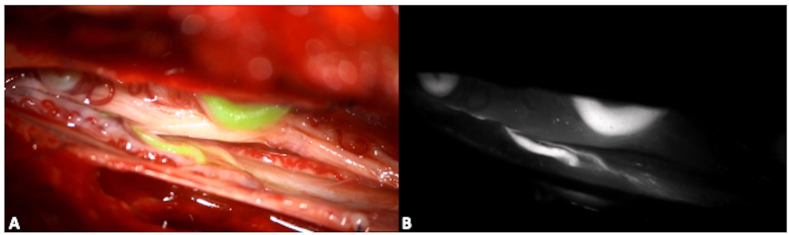
Results: The fundamental mechanisms of action of intraoperative fluorophores are enlightened, examining their interactions with target tissues and the principles driving fluorescence-guided surgery. The clinical applications of the principal fluorophores, namely fluorescein sodium, 5-ALA and indocyanine green, are detailed, in regards to the management of vascular malformations, brain tumors and pathologies treated through endoscopic endonasal approaches.
Discussion and conclusion: Future perspective dealing with the development of new technologies or of new molecules are discussed. By critically assessing the efficacy and applications of the different fluorophores, as well as charting their potential future uses, this paper seeks to guide clinicians in their practice and provide insights for driving innovation and progress in fluorescence-based surgery and research.
Keywords: 5-ALA; Fluorescein sodium; Fluorescence; Fluorophores; Indocyanine green; Microneurosurgery.
© 2024 The Authors.
Conflict of interest statement
None.
Figures
References
-
- Acerbi F., Broggi M., Schebesch K.M., Hohne J., Cavallo C., De Laurentis C., Eoli M., Anghileri E., Servida M., Boffano C., et al. Fluorescein-guided surgery for resection of high-grade gliomas: a multicentric prospective phase II study (FLUOGLIO) Clin. Cancer Res. 2018;24(1):52–61. - PubMed
-
- Akcakaya M.O., Goker B., Kasimcan M.O., Hamamcioglu M.K., Kiris T. Use of sodium fluorescein in meningioma surgery performed under the YELLOW-560 nm surgical microscope filter: feasibility and preliminary results. World Neurosurg. 2017;107:966–973. - PubMed
-
- Albert F.K., Forsting M., Sartor K., Adams H.P., Kunze S. Early postoperative magnetic resonance imaging after resection of malignant glioma: objective evaluation of residual tumor and its influence on regrowth and prognosis. Neurosurgery. 1994;34(1):45–60. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
