

First-in-human trial of atrial fibrillation ablation using real-time tissue optical assessment to predict pulsed field lesion durability
- PMID: 39824175
- PMCID: PMC11832195
- DOI: 10.1093/europace/euaf009
First-in-human trial of atrial fibrillation ablation using real-time tissue optical assessment to predict pulsed field lesion durability
Abstract
Aims: Loss of bipolar electrograms immediately after pulsed field ablation (PFA) makes lesion durability assessment challenging.
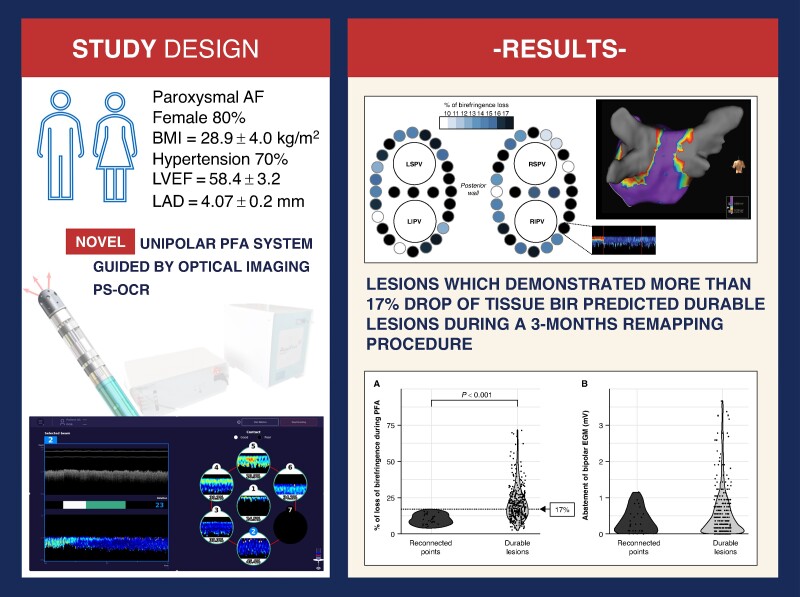
Objective: The aim of this trial (NCT06700226) was to evaluate a novel ablation system that can optically predict lesion durability by detecting structural changes in the tissue during ablation.
Methods and results: Patients with paroxysmal atrial fibrillation underwent pulmonary vein isolation (PVI) using PFA (AblaView®, MedLumics). Using polarization-sensitive optical coherence reflectometry (PS-OCR), reflective characteristics of myocardial tissue and visualization of real-time contrast between healthy tissue and ablated tissue using a drop in tissue birefringence (BiR) was assessed. Wide antral PVI was performed using single point irrigated PFA (unipolar, 1800V, 3 trains, 21 s). Remapping was performed at 3 months. Primary efficacy outcome was the ability of PS-OCR to predict lesion durability at 3-month remapping. Serious adverse events were recorded. Ten patients were included. In total, 38/40 PVs could be isolated with the system. The mean drop of BiR was 17.3 ± 11.5%. Dragging across the ablation lines showed a persistent drop in BiR. During the remap procedures (8/10 patients ablated only with PFA), 12 PVs (37.5%) were found to be electrically reconnected. The mean loss of BiR during all PFA for durable lesions was 20.9%, while only 10.1% BiR loss was observed during the index ablation for reconnected areas (P < 0.001). None of the points with ≥17% loss of birefringence was found to be reconnected.
Conclusion: This first-in-human study supports the use of real-time drop in tissue BiR for lesion assessment and durability during PFA delivery, and its procedural safety.
Keywords: Ablation; Atrial fibrillation; Birefringence; Polarization sensitive optical coherence reflectometry; Pulsed field ablation.
© The Author(s) 2025. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: D.H. and C.B. are employees of MedLumics; A.V. reports grants/advisory from Medtronic, Biosense Webster, Abbott, and advisory from MedLumics and Adagio Medical; R.P.M. reports grants/advisory from Biosense Webster, Abbott, and advisory from MedLumics; G.P. reports advisory fees from MedLumics, A.S. and S.S. report clinical investigators’ fees from MedLumics.
Figures






References
-
- Joglar JA, Chung MK, Armbruster AL, Benjamin EJ, Chyou JY, Cronin EM et al. 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2024;149:e1–156. - PMC - PubMed
-
- Reddy VY, Mansour M, Calkins H, d’Avila A, Chinitz L, Woods C et al. Pulsed field vs conventional thermal ablation for paroxysmal atrial fibrillation: recurrent atrial arrhythmia burden. J Am Coll Cardiol 2024;84:61–74. - PubMed
-
- Dello Russo A, Compagnucci P, Anselmino M, Schillaci V, Campanelli F, Ascione MR et al. Pulsed field vs very high-power short-duration radiofrequency ablation for atrial fibrillation: results of a multicenter, real-world experience. Heart Rhythm 2024;21:1526–36. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
